Rehabilitation Protocol for Reverse Shoulder Arthroplasty
This protocol is intended to guide clinicians and patients through the post-operative course after a reverse shoulder
arthroplasty. Specific interventions should be based on the needs of the individual and should consider exam findings
and clinical decision making. If you have questions, contact the referring physician.
There are a few significant differences in post-operative guidelines between a total shoulder arthroplasty (TSA) and
reverse shoulder arthroplasty (RSA) primarily due to rotator cuff arthropathy. Deltoid function and periscapular strength
become primary sources of shoulder mobility and stability.
Considerations for the Reverse Shoulder Arthroplasty Rehabilitation Program
Many different factors influence the post-operative reverse shoulder arthroplasty rehabilitation outcome, including
surgical approach, concomitant repair of the rotator cuff, arthroplasty secondary to fracture, arthroplasty secondary to
rheumatoid arthritis or osteonecrosis, revision arthroplasty, and individual patient factors including co-morbidities. It is
recommended that patients meet all rehabilitation criteria in order to progress to the next phase and clinicians
collaborate closely with the referring physician throughout the rehabilitation process.
Post-operative Complications
If you develop a fever, unresolving numbness/tingling, excessive drainage from the incision, uncontrolled pain,
unresolving tenderness over the acromion or any other symptoms you have concerns about you should contact the
referring physician.
PHASE I: IMMEDIATE POST-OP (2-3 WEEKS AFTER SURGERY)
Rehabilitation
Goals
• Protect surgical repair
• Reduce swelling, minimize pain
• Maintain UE ROM in elbow, hand and wrist
• Gradually increase shoulder PROM
• Minimize muscle inhibition
• Patient education
Sling
• Neutral rotation
• Use of abduction pillow in 30-45 degrees abduction
• Use at night while sleeping
Precautions
• No shoulder AROM
• No shoulder AAROM
• No shoulder PROM in to IR
• No reaching behind back, especially in to internal rotation
• No lifting of objects
• No supporting of body weight with hands
• Place small pillow/towel roll under elbow while lying on back to avoid shoulder hyperextension
Intervention
Swelling Management
• Ice, compression
Range of motion/Mobility
• PROM: ER in the scapular plane to tolerance, Flex/Scaption </= 120 degrees, ABD </= 90
degrees, seated GH flexion table slide, pendulums, seated horizontal table slides
• AAROM: none
• AROM: elbow, hand, wrist
Criteria to
Progress
• Gradual increase in shoulder PROM
• 0 degrees shoulder PROM in to IR
• Pain < 4/10
• No complications with Phase I
Massachusetts General Hospital Sports Medicine
2
PHASE II: INTERMEDIATE POST-OP (4-6 WEEKS AFTER SURGERY)
Rehabilitation
Goals
• Continue to protect surgical repair
• Reduce swelling, minimize pain
• Gradually increase shoulder PROM
• Initiate shoulder AAROM/AROM
• Initiate periscapular muscle activation
• Initiate deltoid activation (avoid shoulder extension when activating posterior deltoid)
• Patient education
Sling
• Use at night while sleeping
• Gradually start weaning sling over the next two weeks during the day
Precautions
• No reaching behind back, especially in to internal rotation
• No lifting of objects heavier than a coffee cup
• No supporting of body weight with hands
• Place small pillow/towel roll under elbow while lying on back to avoid shoulder hyperextension
Intervention
*Continue with
Phase I
interventions
Range of motion/Mobility
• AAROM: Active assistive shoulder flexion, shoulder flexion with cane, cane external rotation
stretch, washcloth press, seated shoulder elevation with cane
• AROM: supine flexion, salutes, supine punch
Strengthening
• Periscapular: scap retraction, standing scapular setting, supported scapular setting, low row,
inferior glide
• Deltoid: isometrics in the scapular plane
Criteria to
Progress
• Gradual increase in shoulder PROM, AAROM, AROM
• 0 degrees shoulder PROM in to IR
• Palpable muscle contraction felt in scapular musculature
• Pain < 4/10
• No complications with Phase II
PHASE III: INTERMEDIATE POST-OP CONTD (7-8 WEEKS AFTER SURGERY)
Rehabilitation
Goals
• Minimize pain
• Gradually progress shoulder PROM, initiate shoulder PROM IR in the scapular plane
• Gradually progress shoulder AAROM
• Gradually progress shoulder AROM
• Progress deltoid strengthening
• Progress periscapular strengthening
• Initiate motor control exercise
• Patient education
Sling
• Discontinue
Precautions
• No reaching behind back beyond pant pocket
• No lifting of objects heavier than a coffee cup
• No supporting of body weight with hands
• Avoid shoulder hyperextension
Intervention
*Continue with
Phase I-II
interventions
Range of motion/Mobility
• PROM: Full in all planes, gradual PROM IR in scapular plane </=50 degrees
• AAROM: incline table slides, wall climbs, pulleys, seated shoulder elevation with cane with active
lowering
• AROM: seated scaption, seated flexion, supine forward elevation with elastic resistance to 90 deg
Strengthening
• Periscapular: Row on physioball, serratus punches
• Deltoid: seated shoulder elevation with cane, seated shoulder elevation with cane with active
lowering, ball roll on wall
Motor control
• IR/ER in scaption plane and Flex 90-125 (rhythmic stabilization) in supine
Stretching
• Sidelying horizontal ADD, triceps and lats
Massachusetts General Hospital Sports Medicine
3
Criteria to
Progress
• ROM goals**:
o Elevation </= 140 degrees
o ER </= 30 degrees in neutral
o IR </= 50 degrees in scapular plane or back pocket
o **PROM and AROM expectations are individualized and dependent upon ROM measurements
attained in the OR post-operatively
• Minimal to no substitution patterns with shoulder AROM
• Pain < 4/10
PHASE IV: TRANSITIONAL POST-OP (9-11 WEEKS AFTER SURGERY)
Rehabilitation
Goals
• Maintain pain-free ROM
• Progress periscapular strengthening
• Progress deltoid strengthening
• Progress motor control exercise
• Improve dynamic shoulder stability
• Gradually restore shoulder strength and endurance
• Return to full functional activities
Precautions
• No lifting of heavy objects (> 10 lbs)
Intervention
*Continue with
Phase II-III
interventions
Range of motion/mobility
• PROM: Full ROM in all planes
Strengthening
• Periscapular: Resistance band shoulder extension, resistance band seated rows, rowing, robbery,
lawnmowers, tripod, pointer
• Deltoid: gradually add resistance with deltoid exercise
Motor control
• IR/ER and Flex 90-125 (rhythmic stabilization)
• Quadruped alternating isometrics and ball stabilization on wall
• Field goals
• PNF – D1 diagonal lifts, PNF – D2 diagonal lifts
Criteria to
Progress
• Performs all exercises demonstrating symmetric scapular mechanics
• Pain < 2/10
PHASE V: ADVANCED STRENGTHENING POST-OP (12-16 WEEKS AFTER SURGERY)
Rehabilitation
Goals
• Maintain pain-free ROM
• Initiate RTC strengthening with a concomitant repair
• Improve shoulder strength and endurance
• Enhance functional use of upper extremity
Precautions
• No lifting of objects (> 15 lbs)
Intervention
*Continue with
Phase II-IV
interventions
Strengthening
• Periscapular: Push-up plus on knees, “W” exercise, resistance band Ws, prone shoulder extension
Is, dynamic hug, resistance band dynamic hug, resistance band forward punch, forward punch, T
and Y, “T” exercise
• Deltoid: continue gradually increasing resisted flexion and scaption in functional positions
• Elbow: Bicep curl, resistance band bicep curls, and triceps
• Rotator cuff: internal external rotation isometrics, side-lying external rotation, Standing external
rotation w/ resistance band, standing internal rotation w/ resistance band, internal rotation,
external rotation, sidelying ABD→standing ABD
Motor Control
• Resistance band PNF pattern, PNF – D1 diagonal lifts w/ resistance, diagonal-up, diagonal-down,
wall slides w/ resistance band
Criteria to
Progress
• Clearance from MD and ALL milestone criteria have been met
• Maintains pain-free PROM and AROM
• Performs all exercises demonstrating symmetric scapular mechanics
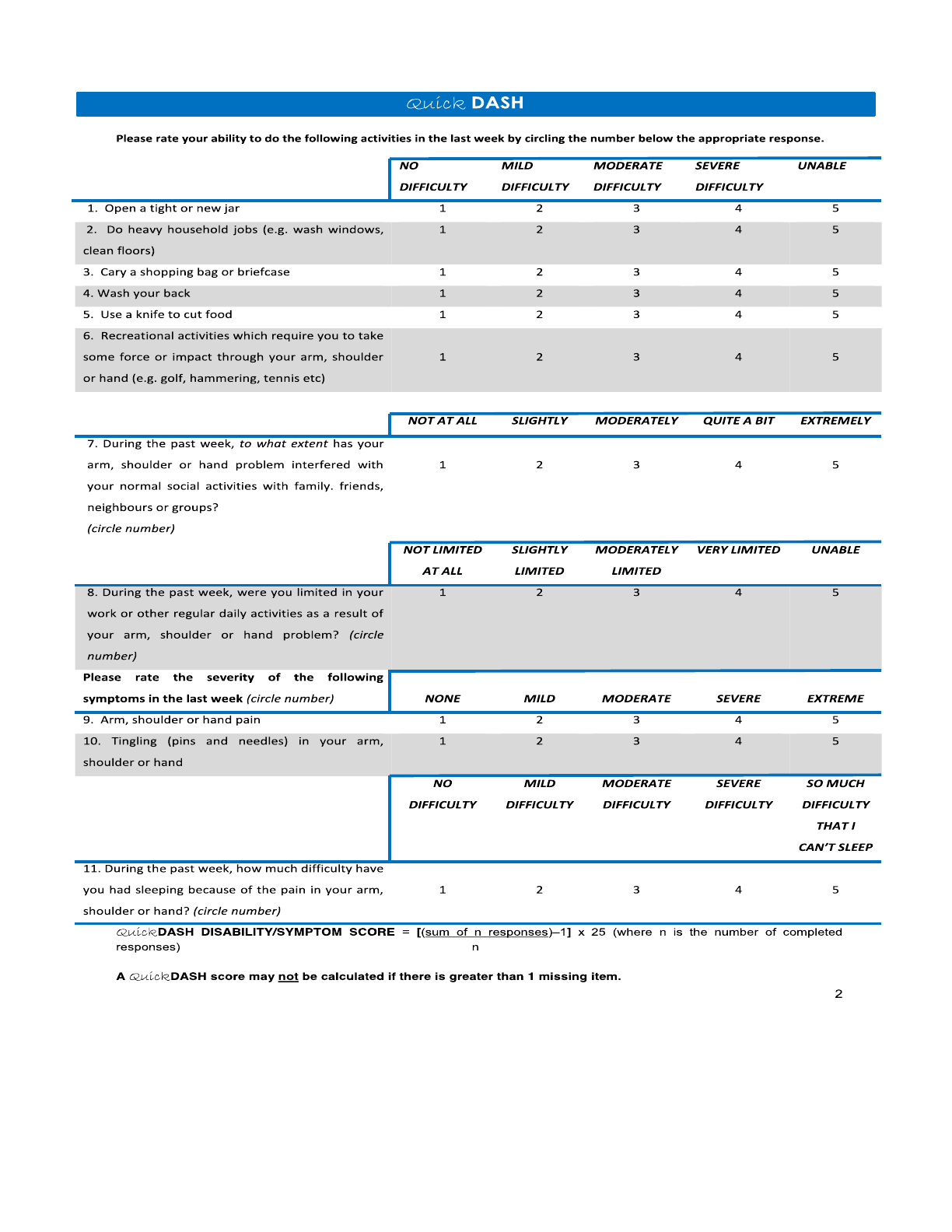
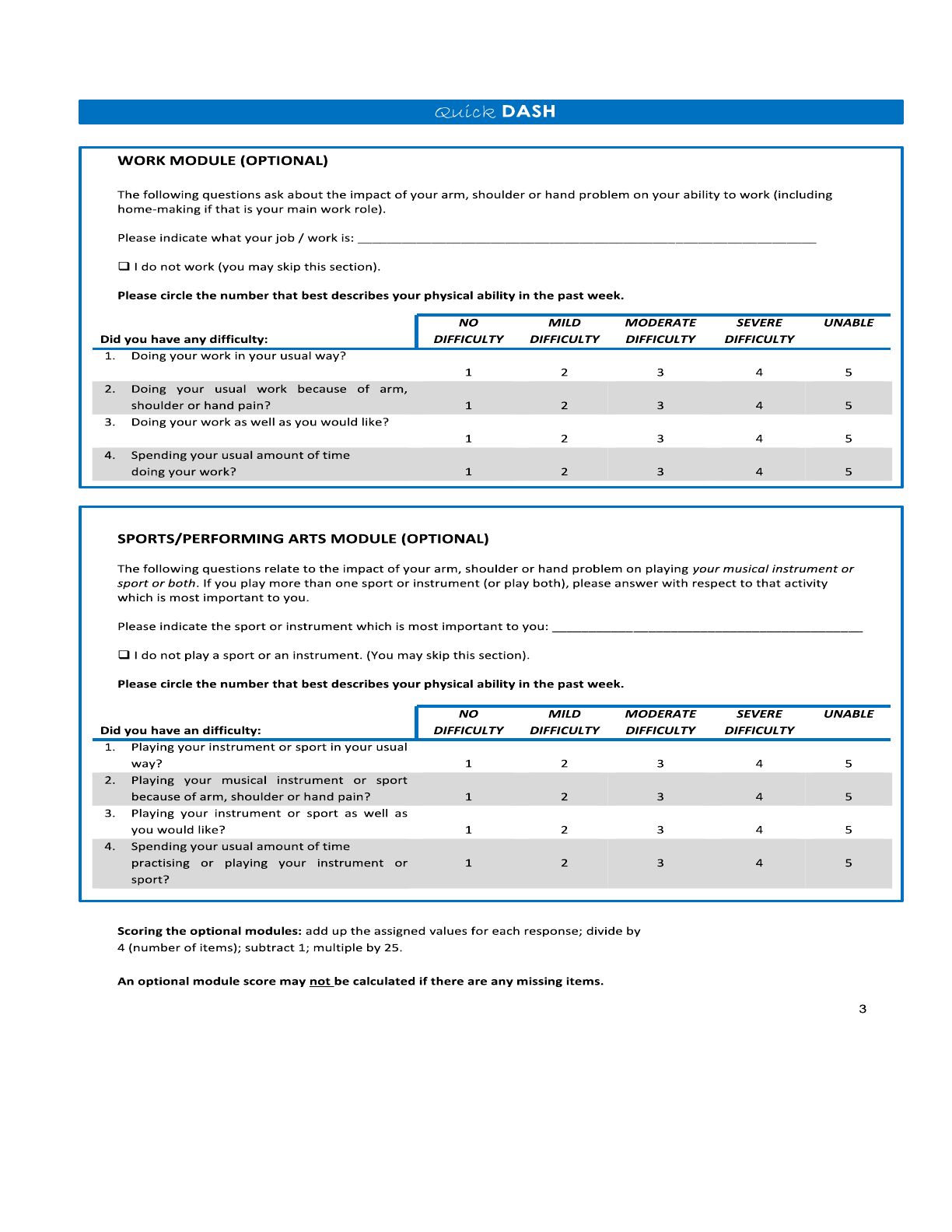
• QuickDASH
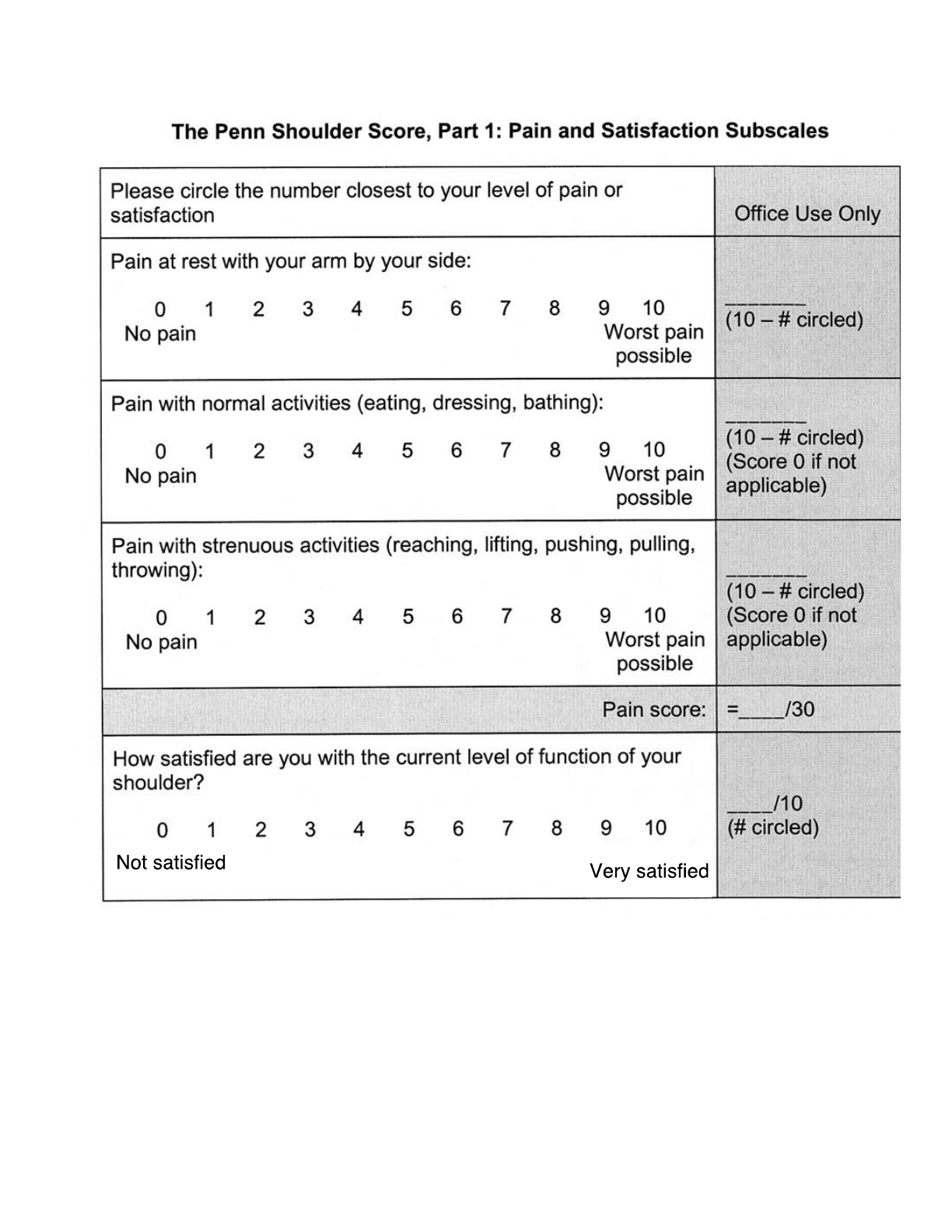
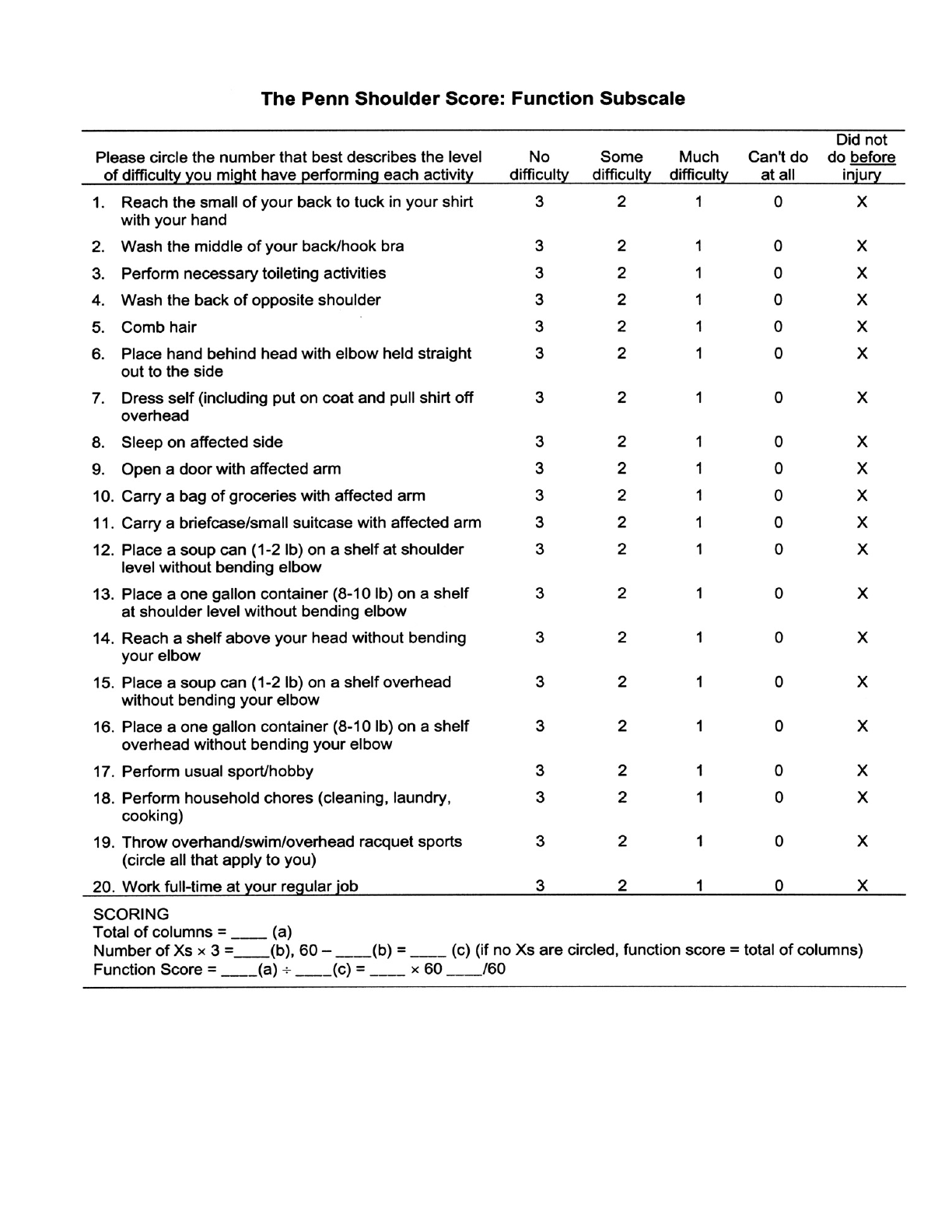
• PENN

Massachusetts General Hospital Sports Medicine
4
Revised December 2018
Contact
Please email MGHSportsPhysica[email protected] with questions specific to this protocol
References
Angst F, Goldhahn J, et al. Responsiveness of six outcome assessment instruments in total shoulder arthroplasty. Arthritis & Rheumatism. 2008. 59 (3): 391-398.
Boudreau S, Boudreau E. Higgins LD, Wilcox III R.B. Rehabilitation following reverse total shoulder arthroplasty. JOSPT. 2007. 37 (12): 734-744.
Garcia GH, Taylor SA, et al. Patient activity level after reverse total shoulder arthroplasty: what are patients doing? Am J of Sports Med. 2015. 43 (11): 2816-2821.
Gaunt BW, McCluskey GM, Uhl TL. An electromyographic evaluation of subdividing active-assistive shoulder elevation exercises. Sports Health. 2010. 2 (5): 424-432.
Hughes M, Neer II CS. Glenohumeral joint replacement and postoperative rehabilitation. Physical Therapy. 1975. 55(8): 850-858.
Kibler WB, Sciascia, AD, Uhl, TL, et al. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. The American
Journal of Sports Medicine. 2008. 36(9): p. 1789-1798.
Knesek M, Brunfeldt A, et al. Patterns of strain and the determination of the safe arc of motion after subscapularis repair-a biomechanical study. Journal of Orthopaedic
Research. 2016. 34: 518-524.
Piasecki DP, Nicholson GP. Tears of the subscapularis tendon in athletes-diagnosis and repair techniques. Clin Sports Med. 2008. 27: 731-745.
Uhl TL, Muir TA, et al. Electromyographical assessment of passive, active assistive, and active shoulder rehabilitation exercises. PM R. 2010. 2: 132-141.
Wolff AL, Rosenzweig L. Anatomical and biomechanical framework for shoulder arthroplasty rehabilitation. Journal of Hand Therapy. 2017. 30: 167-174.
Wright T, Easley T, et al. Shoulder arthroplasty and its effect on strain in the subscapularis muscle. Clinical Biomechanics. 2015. 30: 373-376.
Massachusetts General Hospital Sports Medicine
5
Massachusetts General Hospital Sports Medicine
6
Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative
Group (UECG). Am J Ind Med. 1996;(6):602-608.
Massachusetts General Hospital Sports Medicine
7
Massachusetts General Hospital Sports Medicine
8
Leggin BG, Michener, LA, et al. The Penn Shoulder Score: reliability and validity. JOSPT. 36 (3): 138-151.
