
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
1
Total Shoulder Arthroplasty
The intent of this resource is to provide clinicians with a general guideline of the
post-operative rehabilitation of patients undergoing a total shoulder arthroplasty
(TSA). This guideline is not intended to mandate the course of patient care. If
there are concerns regarding the patient’s clinical presentation, please consult
and collaborate with your colleagues and the referring physician as needed.
Progression through this guideline as well as overall expected goals are ultimately
determined by the pathology that led to the need of the TSA ranging from
osteoarthritis, rheumatoid arthritis, humeral fracture, etc. A review of the
patient’s past medical history and operative notes to determine the technique
that was used to complete the TSA (i.e. lesser tuberosity osteotomy, subscapularis
peel, or subscapularis tenodesis). Knowing your patient’s prior level of function
will also be helpful in establishing appropriate goals for the patient. A full course
of post-operative physical therapy for this patient population is between 4-6
months depending on the specific surgical interventions. Total recovery time
could be 12-18 months. While many may not regain full range of motion, most are
expected to achieve functional mobility. Outcome will depend on the patient’s
past medical history, pathology necessitating the TSA, and individual functional
goals. Virtual visits are appropriate for treatment sessions for this patient
population while completing assessments in person.
Background Information
In order to best use this guideline as part of your clinical decision-making process,
it is important to understand the various surgical techniques including what
anatomical structures are involved. This information as well as a familiarity with
current literature will help clinicians provide the best possible care for successful
rehabilitation. Typically, a TSA is performed through the deltopectoral interval,
and the surgeons visualize and access the glenohumeral joint through either a
lesser tuberosity osteotomy, subscapularis peel, or subscapularis tenodesis.

Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
2
Knowing which approach was performed is vital to a patient’s prognosis as
subscapularis dysfunction is associated with pain, weakness, and/or anterior
instability and ultimately failure. While studies have shown no significant
biomechanical difference between these techniques,
1
others have shown that
load-to-failure force of the repair is stronger with a lesser tuberosity osteotomy.
2
This may be due to bone-to-bone healing in the lesser tuberosity osteotomy
requiring less healing time which allows for acceleration of exercise progressions.
This process is theoretically slower for tendon-to-bone healing at the lesser
tuberosity involved in a subscapularis peel or tendon-to-tendon healing in a
subscapularis tenodesis.
Complication rates are low following TSA but range from anterosuperior
instability due to poor subscapularis function, posteroinferior instability, superior
rotator cuff tears, broken screws, and implant loosening.
3
,
4
If a subscapularis
repair is involved, studies have shown a failure rate between 13 and 47%.
5
According to Singh et al., the implant survivorship rate at 20 years is 81%.
6
Certain
factors that may affect patient success include medical history such as slowed
healing times due to diabetes and osteoporosis as well as lifestyle choices
including smoking.
Regardless of the technique of surgery performed, understanding the importance
of subscapularis healing in the rehabilitation process is important to a patient’s
success. However, there is no consensus in the literature on what that means for
the timing of progressions. In the first stage of post-operative care, it is important
to minimize subscapularis muscle activation and stress to allow for proper
healing. Therefore, exercise should be passive and limited in planes of motion. A
2016 study by Denard and Lätterman concluded that there were minimal negative
outcomes after delaying range of motion (ROM) to at least four weeks post-
operatively to allow for subscapularis healing while there is a risk of failure from a
lack of full tissue healing with immediate ROM.
7
Furthermore, studies have shown
no difference in long-term shoulder function between immediate and delayed
ROM.
8
A 2014 study suggested that prolonged immobilization is important for
older patients or for those who had larger cuff tears.
9
EMG studies have shown
minimal general muscle activation with small-diameter pendulums if performed
correctly,
10
as well as with passive flexion with table slides,
11
a cane, and manual

Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
3
PROM.
12
,
13
Other EMG studies demonstrated that pulley exercises are not passive
and therefore place healing tissue under increased stress.
14
,
15
Muraki et al. found
the greatest strain on the subscapularis in external rotation especially in
abduction.
16
Furthermore, it is vital to teach patients how to properly don and
doff a sling as studies have shown high subscapularis activity in these
movements.
17
Patients should also limit other independent movements during
activities of daily living (ADLs) to allow for subscapularis healing including avoiding
tucking in the back of a shirt, reaching into a back pocket, and reaching to
contralateral axilla as with bathing.
18
Patients can advance to the next rehabilitation stage if their pain is minimal and if
their motor control is optimal. Studies show that scapulothoracic motion
contributes significantly to shoulder motion following TSA, so periscapular
strengthening is important to promote scapular control while minimizing stress in
the glenohumeral joint.
19
Deltoid, rotator cuff, and periscapular muscle
strengthening can begin once maximal functional ROM has been achieved and
based on the stages of tissue healing.
Later stages of post-operative rehabilitation are focused on strengthening and
regaining function. Gaunt et al.
demonstrated that maximum muscle activation of
the supraspinatus, infraspinatus, and anterior deltoid occurs with upright active
flexion,
20
and Cahill et al. highlighted that at 90 degrees of elevation, the force
through the glenohumeral joint is about ten times the weight of the upper
extremity.
21
Furthermore, much of the research done for rotator cuff repairs
suggests that loaded exercises should not be started earlier than 12 weeks to
allow for sufficient bone-to-tendon healing and integration.
22
When a patient is
pain-free, has good motor control, and has met other necessary requirements, it
is important to gradually introduce active and strengthening exercises.
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
4
These time frames are just examples and can be adjusted based on the given procedure
Progression to the next phase based on achieving both Clinical Criteria as well as Time Frames. Variance from
this needs to be reviewed with surgeon. Suggestions for home exercise program (HEP) provided.
Phase I – Immediate Post-Surgical Phase (Day 1)
Goals
- Understanding how to don/doff sling
- Understanding activity restrictions for proper soft tissue healing
- Reduce pain and inflammation
Precautions
- Sleeping (6-8 weeks): wear sling with a small pillow or towel roll under entire upper arm
to avoid shoulder hyperextension and resulting strain on subscapularis as well as anterior
capsule
- Keep incision clean and dry (no soaking for 2 weeks)
Things to avoid
- Active range of motion (AROM)
- Weight-bearing through involved extremity (i.e. pushing up from seated position, rolling
over in bed, etc.)
Criteria for
progression to
the next phase
- Understands importance of sling use and adhering to instructions
- Avoids active movements to ensure proper soft tissue healing
- Independent in donning and doffing sling
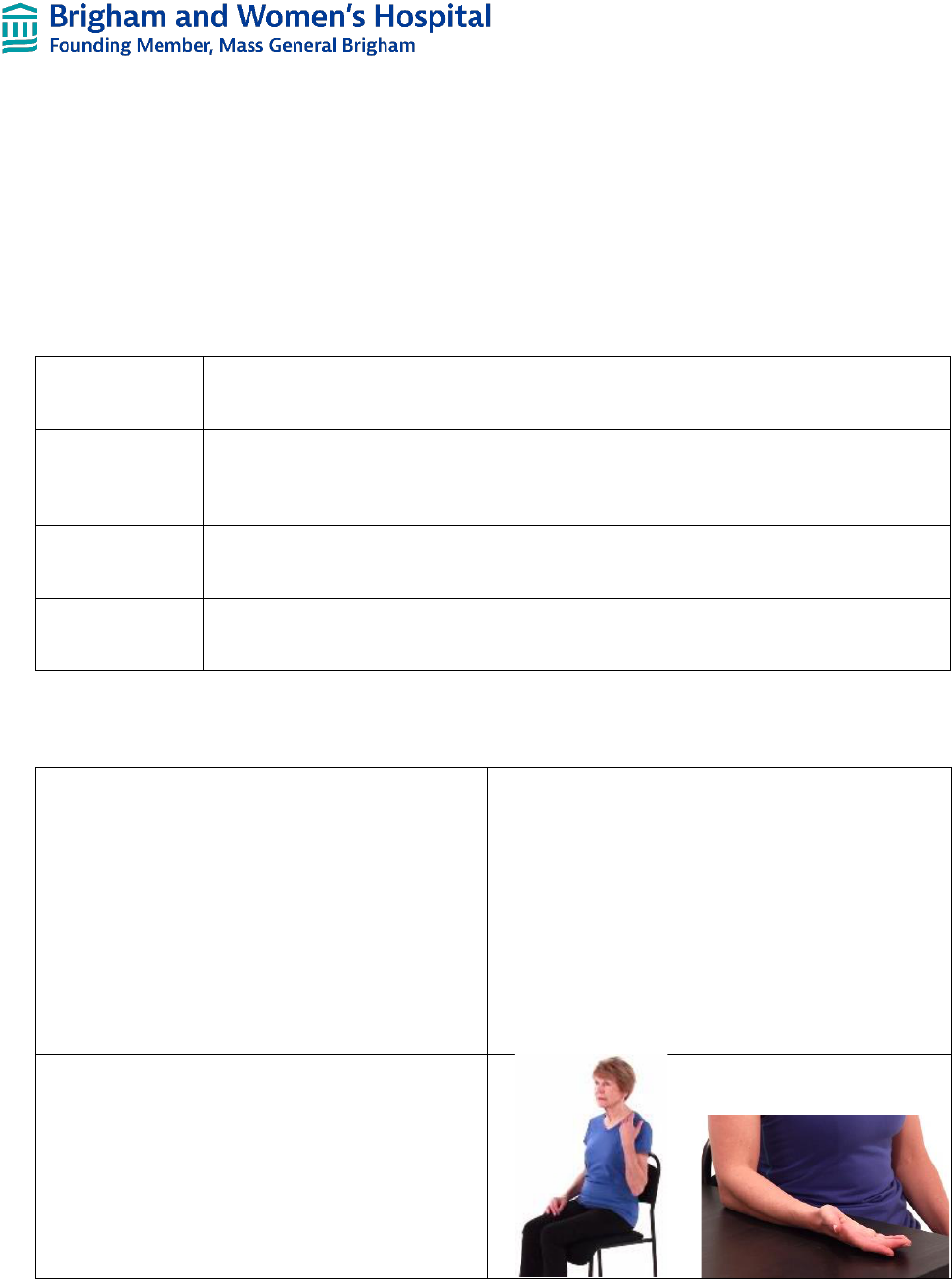
Interventions:
Sling, immobilization strap, and/or abduction pillow
use
• Type per surgeon preference based on
surgical intervention
• Worn for 4-6 weeks depending on surgical
procedure and underlying pathology
necessitating TSA
• Can be removed for showering and to
complete rehabilitation home exercises
Elbow/Forearm AROM
• With upper arm at patient’s side
• Elbow flexion and extension focusing on full
ROM
• Forearm pronation and supination
• HEP: to be completed multiple times a day
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
5
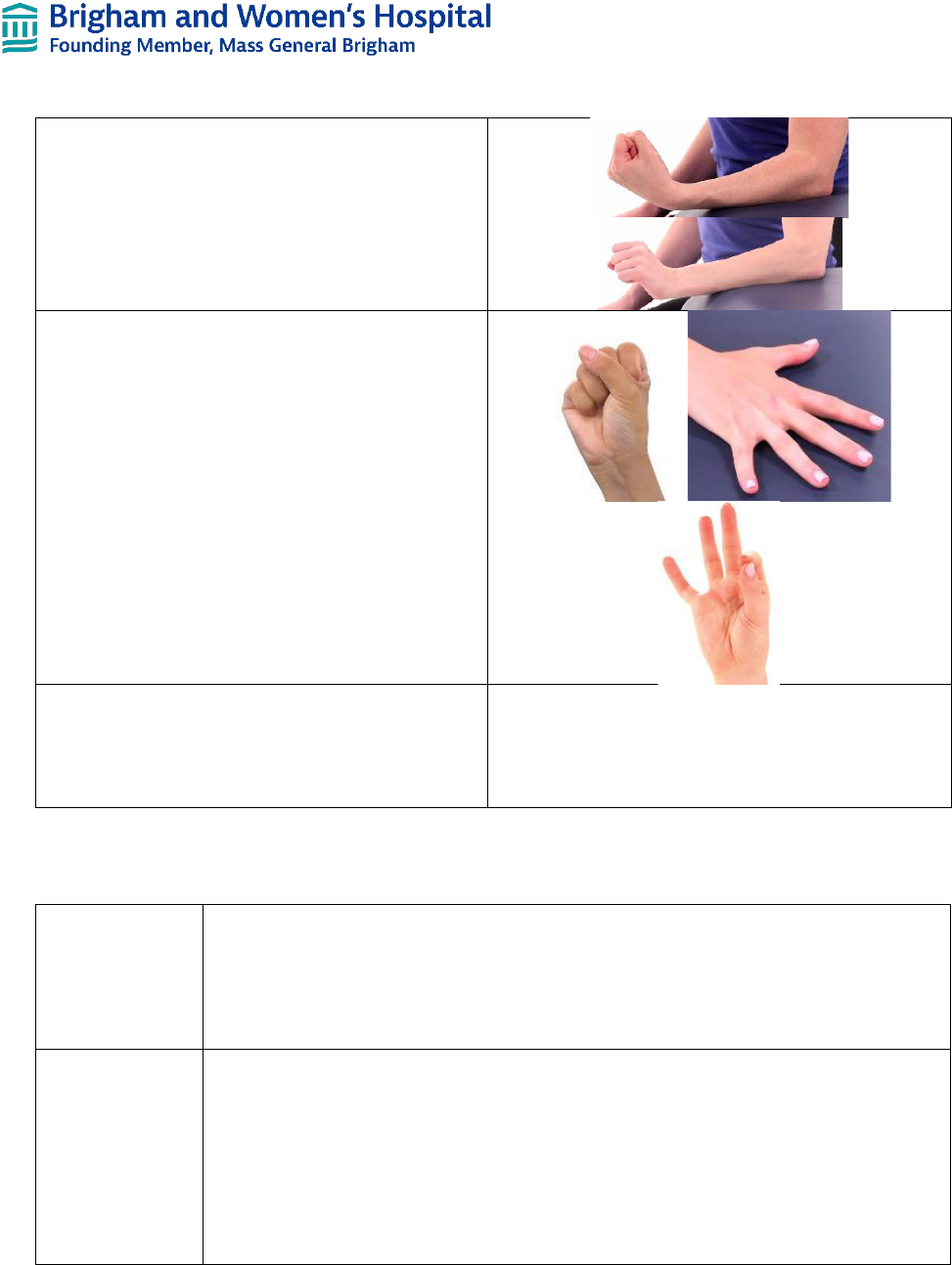
Wrist AROM
• With arm in sling or supported on table
• Wrist flexion, extension, ulnar deviation, and
radial deviation
• Wrist circles
• HEP: to be completed 3-5x a day
Hand/Finger AROM
• With arm in sling or supported on table
• Finger flexion and extension at every joint
• Gentle gripping activities
• HEP: to be completed 3-5x a day
Cryotherapy
• To control pain
• HEP: can be complete multiple times a day
15-20 minutes
Phase II – Protection Phase (Day 2 - Week 6)
Goals
- Allow for soft tissue healing
- Protect subscapularis tenodesis or lesser tuberosity osteotomy
- Reduce muscular guarding
- Become independent with ADLs, bed mobility, and transfers with modifications as needed
while wearing the sling
- Restore active range of motion elbow, wrist, and hand
Precautions
- Continued use of sling including when sleeping except when showering and with PT and
home exercises
- Light, pain-free ADLs only with modifications as needed (i.e. brushing teeth, dressing,
etc.)
- Keep incision clean and dry (no soaking for 2 weeks)
- Shoulder external rotation (ER) PROM limited to at most 20° to prevent passive tension
on repaired subscapularis tendon especially in abduction
- Shoulder internal rotation (IR) AROM and resisted exercises limited to prevent tension in
repaired subscapularis tendon
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
6
Things to avoid
- Shoulder AROM (At 90° of elevation, the force through the glenohumeral joint is about
ten times the weight of the extremity; therefore, do not start active elevation too early to
allow for proper soft tissue healing)
- Stress on anterior shoulder
- Excessive shoulder motion behind the back especially into IR
- Excessive stretching or sudden movements especially into ER
- Painful ADLs
- Lifting activities (including drinking if subscapularis involved in surgery)
- Driving while in sling for 4-6 weeks
- Weight-bearing through involved extremity (i.e. pushing up from seated position, rolling
over in bed, etc.)
Criteria for
progression to
the next phase
- Minimal pain
- Flexion PROM at least 120°
- ER PROM 15-20°
NOTE: If the patient has not reached the above ROM, forceful stretching, PROM, and/or mobilization/manipulation
are not indicated. Continue with gradual ROM and mobilizations (Gr II for pain control and Gr III-IV for ROM and
capsular restrictions) while respecting soft tissue constraints.
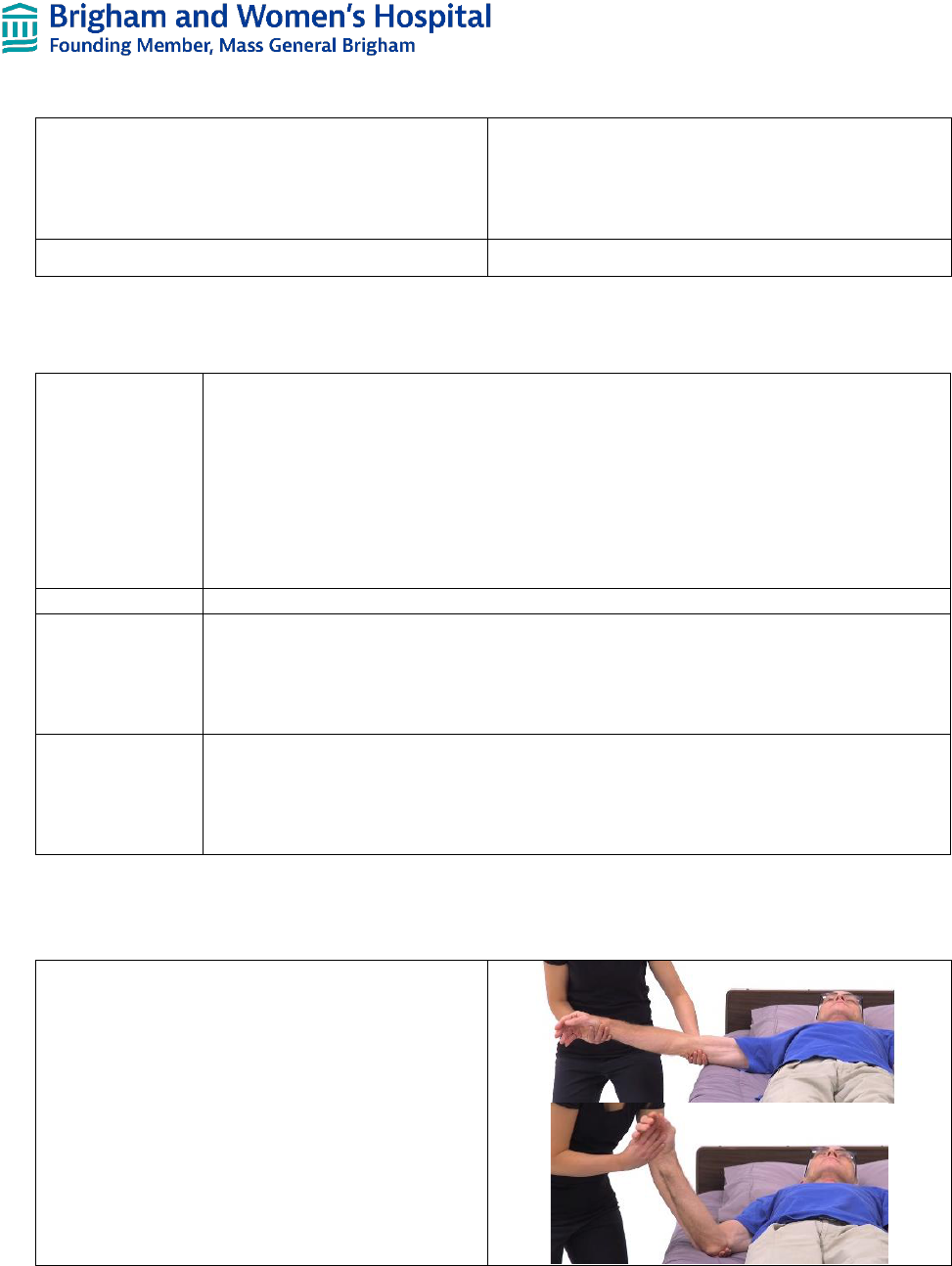
Interventions (1 PT treatment session every 1-2 weeks including virtual visits):
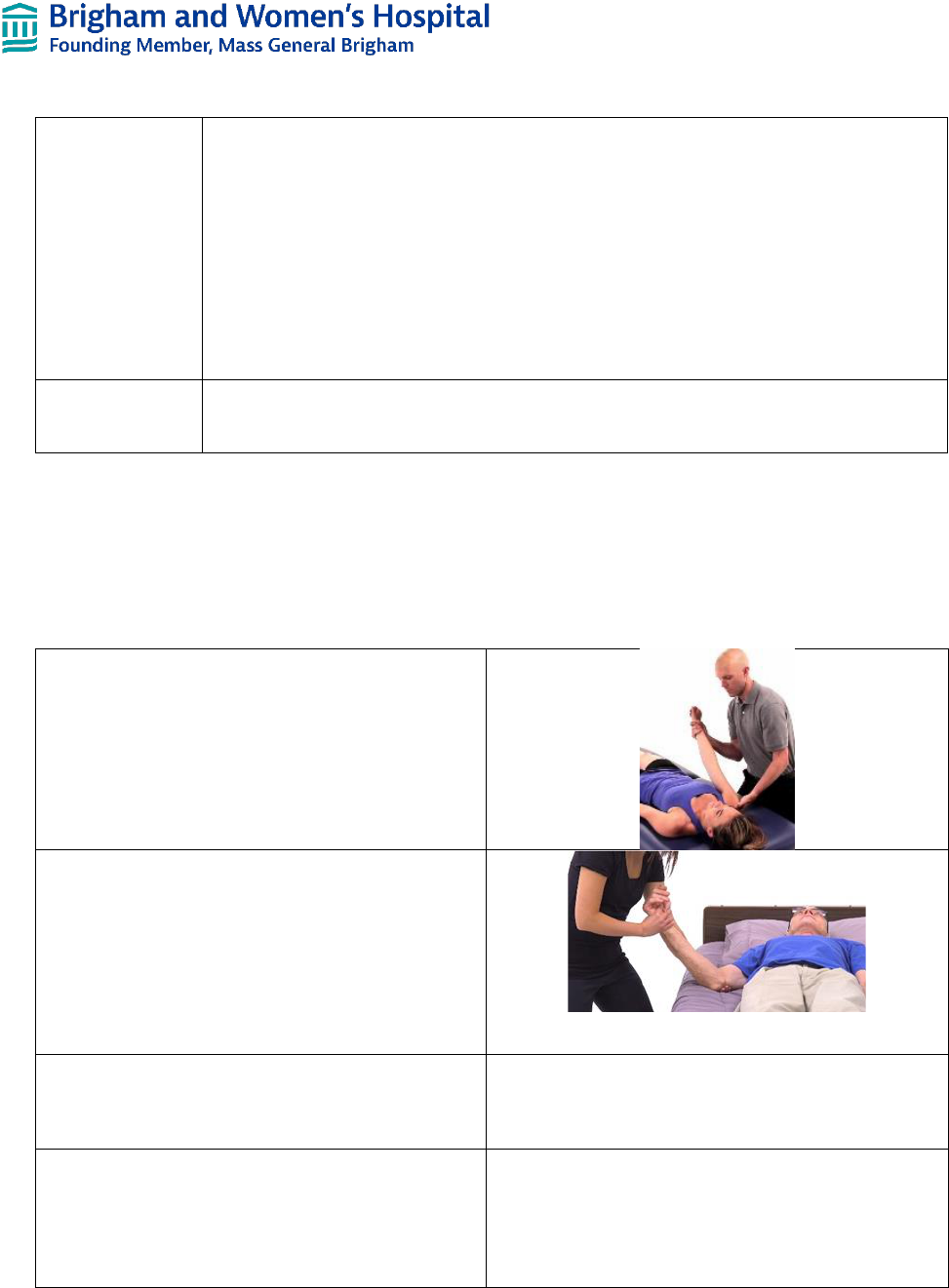
PROM – Flexion and scaption
• In pain-free ROM
• Without placing undue stress on the soft
tissue structures or surgical repair
• Avoid stretching
PROM – ER
• To be started in weeks 4-6
• Through pain-free ROM
• To neutral at first to counter prolonged sling
use or to 20 degrees depending on surgical
approach
Scapulothoracic mobilizations
• With upper extremity supported in scapular
plane and neutral rotation
Glenohumeral Joint mobilizations
• Grade I-II for pain control
• Avoid overstraining anterior shoulder
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
7
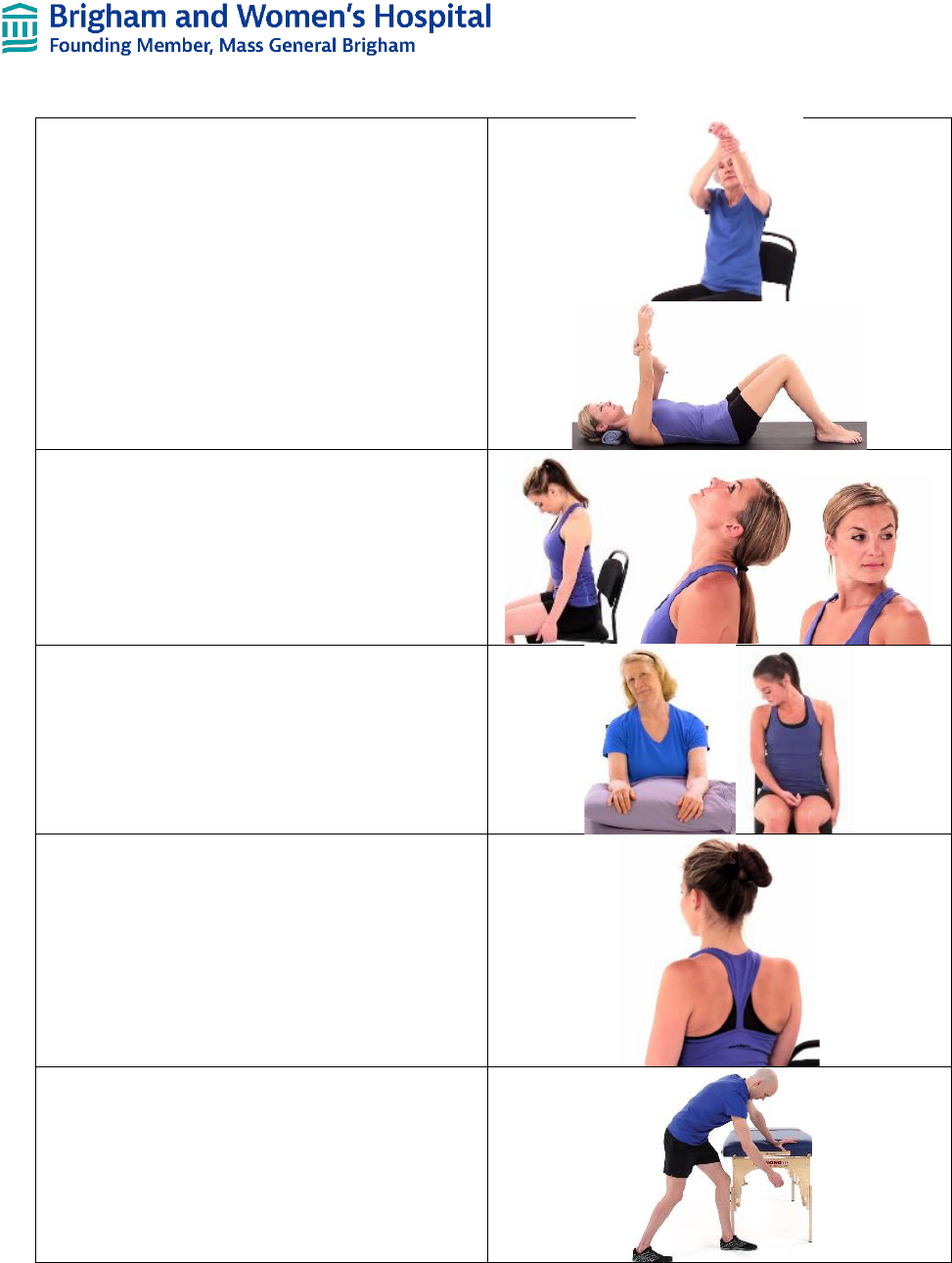
AAROM – Flexion
• In supine and sitting
• Through pain-free ROM
• HEP: to be completed 3-4x a day
Cervical AROM
• Through pain-free ROM
• Chin tucks in supine, sitting, and/or standing
• HEP: to be completed 2x a day
Cervical muscle stretches: upper trapezius, levator,
and scalenes
• Into pain-free range of motion
• Bilateral
• 3x30 second holds
• HEP: to be completed 2x a day
Scapular retractions
• With arm in sling and sitting in good posture
• Performed gently and through comfortable
ROM without straining anterior shoulder
structures
• HEP: to be completed 3-4x a day
Pendulums
• For muscle relaxation
• Discourage large movement to avoid
activation of rotator cuff muscles
• HEP: to be completed 3-4x a day
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
8
Continue Elbow/Forearm and Hand/Wrist/Finger
AROM from previous stage
• HEP: to be completed 2x a day
Continue Cryotherapy
Phase III – Intermediate Phase (Weeks 6-10)
Goals
- Maximize ROM while allowing continued healing especially of the subscapularis or lesser
tuberosity osteotomy
- Optimize neuromuscular control
- Improve scapular strength
- Gradually weaning off sling excluding in uncontrolled environments (i.e. in crowds,
around dogs, etc.) for protection
- Be able to perform light ADLs independently and without pain
- Demonstrate the ability to isometrically activate all components of the deltoid as well as
scapular musculature
Precautions
- Repetitive active motions
Things to avoid
- Painful or more strenuous ADLs
- ADLs involving reaching into extension and IR causing stress to anterior shoulder
structures (i.e. reaching into back pocket, tucking in back of shirt, etc.)
- Lifting anything heavier than a cup of coffee
- Weight bearing through involved arm
Criteria for
progression to
the next phase
- Tolerates advanced PROM program
- Tolerates isometric program for muscle activation
- Flexion AROM 90° in standing with normal scapulohumeral mechanics
- Flexion PROM at least 140°
- ER PROM 30°
Interventions (1 PT treatment session every 1-2 weeks including virtual visits):
PROM – Flexion, scaption, ER, and abduction
• ER to be completed in neutral or scapular
plane
• Avoid increasing abduction as greatest strain
on subscapularis is with ER at 90 degrees
abduction
• In pain-free ROM
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
9
Continue Scapulothoracic mobilizations from
previous stage
Continue Glenohumeral Joint mobilizations from
previous stage
• Grade III-IV for ROM and capsular
restrictions
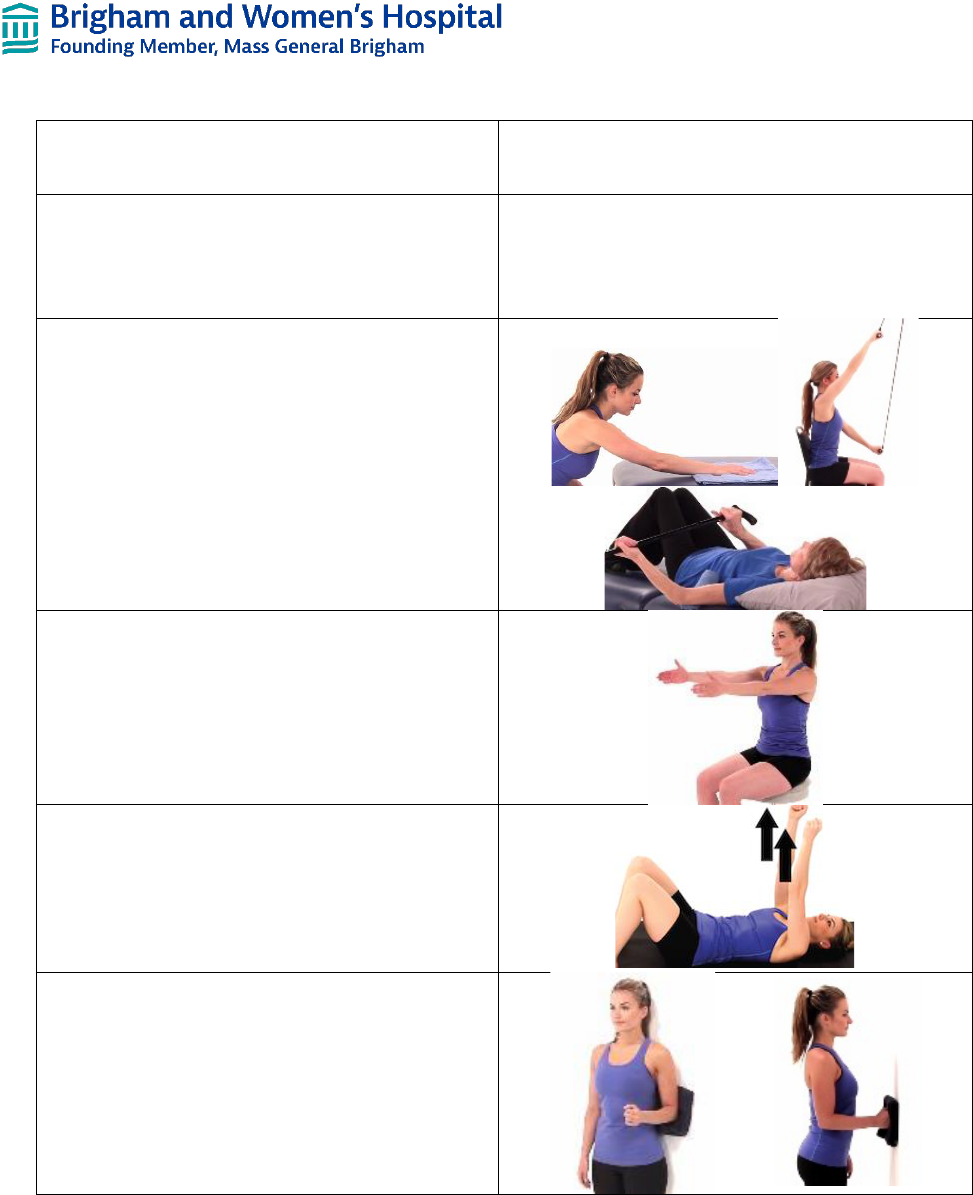
AAROM – Flexion, scaption, ER, and abduction
• In pain-free range of motion
• Start with cane, table slides, etc.; then added
pulleys
• HEP: to be complete 3-4x a day for short hold
(times 2-3 seconds)
AROM – Flexion and scaption
• In pain-free ROM
• Focus on proper scapulohumeral rhythm and
body mechanics
• HEP: to be completed 2-3x a day for short
hold times (2-3 seconds)
Postural Exercises – Supine Serratus Anterior
Protraction
• Focus on eccentric scapular control on return
to start
• HEP: to be completed 2-4x a day
Isometrics – Deltoids
• Flexion and extension
• Submaximal pressure
• Pain-free
• 5 second holds
• HEP: to be completed 2-4x a day
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
10
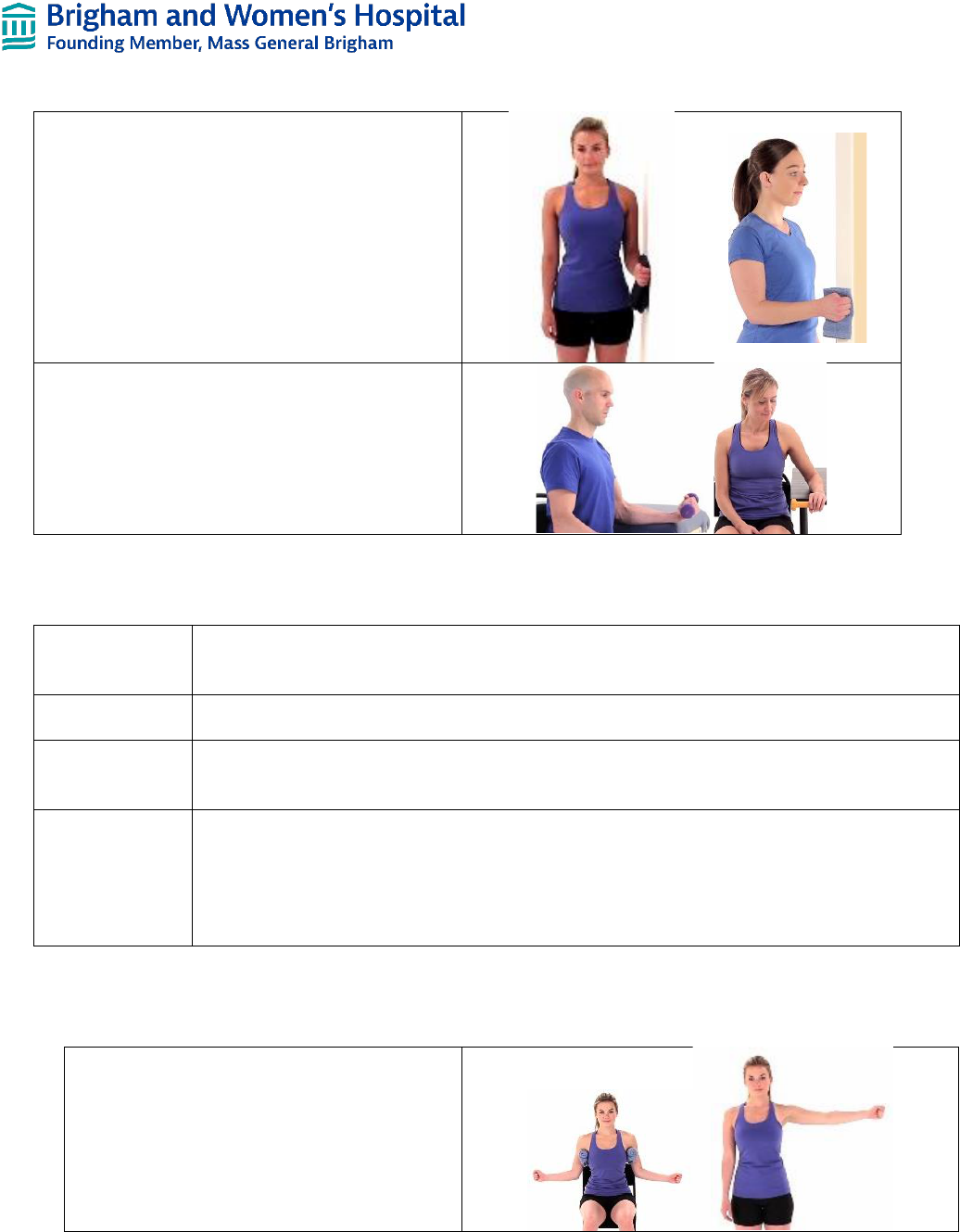
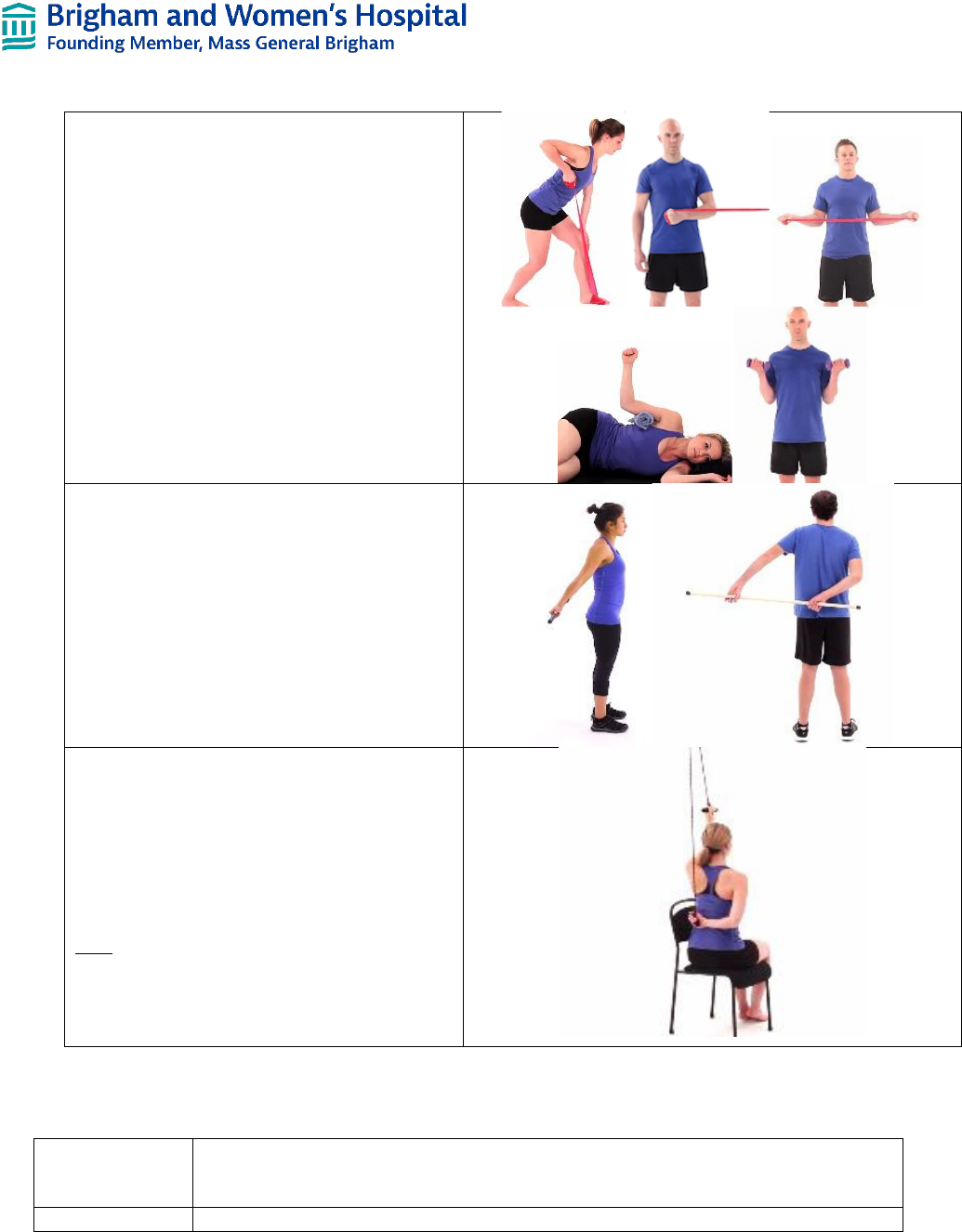
Isometrics – ER and IR
• To be completed initially starting at doorway
• Submaximal pressure
• Pain-free
• 5 second holds
• Progress to stepping against resistance band
at or after week 8
• HEP: to be completed 2x a day
Distal upper extremity strengthening
• Wrist flexion, extension, ulnar and radial
deviations, as well as forearm supination and
pronation
• Start with 1-3# hand weights
• HEP: to be completed 1x a day
Phase IV – Advanced Strengthening Phase (Week 10-16)
Goals
- Gradual increase in AROM
- Gradual return to functional activities
- Improve muscle strength and endurance
Precautions
- Repetitive shoulder exercises especially AROM in standing against gravity in the presence of poor
shoulder mechanics
Things to avoid
- Heavy lifting greater than 10#
- Sudden, jerking motions
- Heavy pushing or pulling motions
Criteria for
progression to
the next phase
- Functional/full ROM
- Flexion AROM at least 140° in supine and at least 120° in standing with good scapulohumeral
rhythm
- Flexion PROM 160°
- ER PROM 60°
- NOTE: if patient is limited in flexion ROM, use Levy Lawn Chair Progression Protocol
Interventions (1 PT treatment session a week):
AROM – all planes of motion
• Pain-free
• Focus on body mechanics
• HEP: to be completed 2-3x a day for
short holds times (2-3 seconds)
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
11
Manual Rhythmic Stabilizations
• Patient in supine or standing (i.e. ball on
table, wall, etc.)
• Flexion
• IR/ER in 0° of elevation
• Submaximal and pain-free
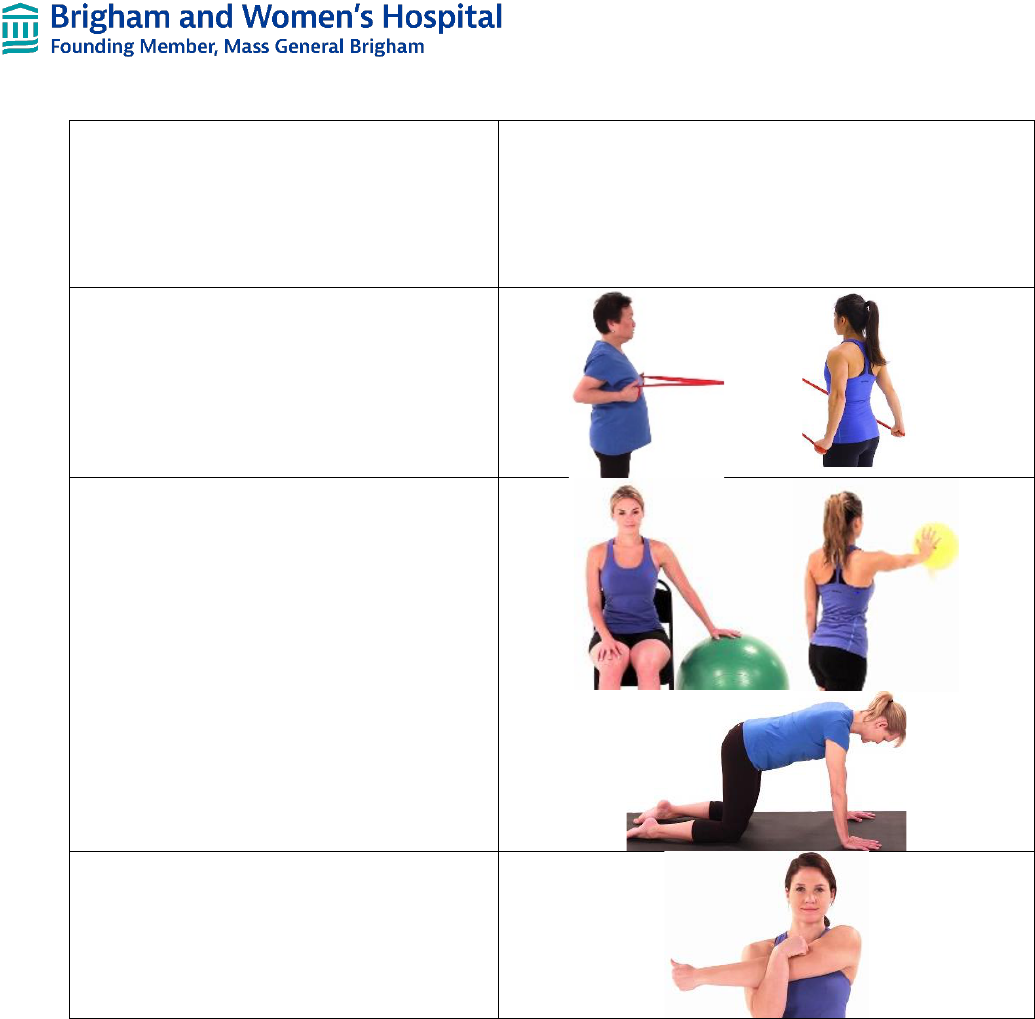
Postural Strengthening
• Focus on body mechanics
• Rows with resistance bands
• Extensions with resistance bands
• HEP: to be completed 1-2x a day
Weight Bearing Exercises
• To be started at or after week 12
• Weight shifting, table/wall ball rolls, etc.
and gradually progress to quadruped
• To improve scapular stability
• HEP: to be completed 1-2x a day
Stretching – Posterior Capsule Stretch
• In pain-free ROM
• 3x30 second holds
• HEP: to be completed 2-3x a day
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
12
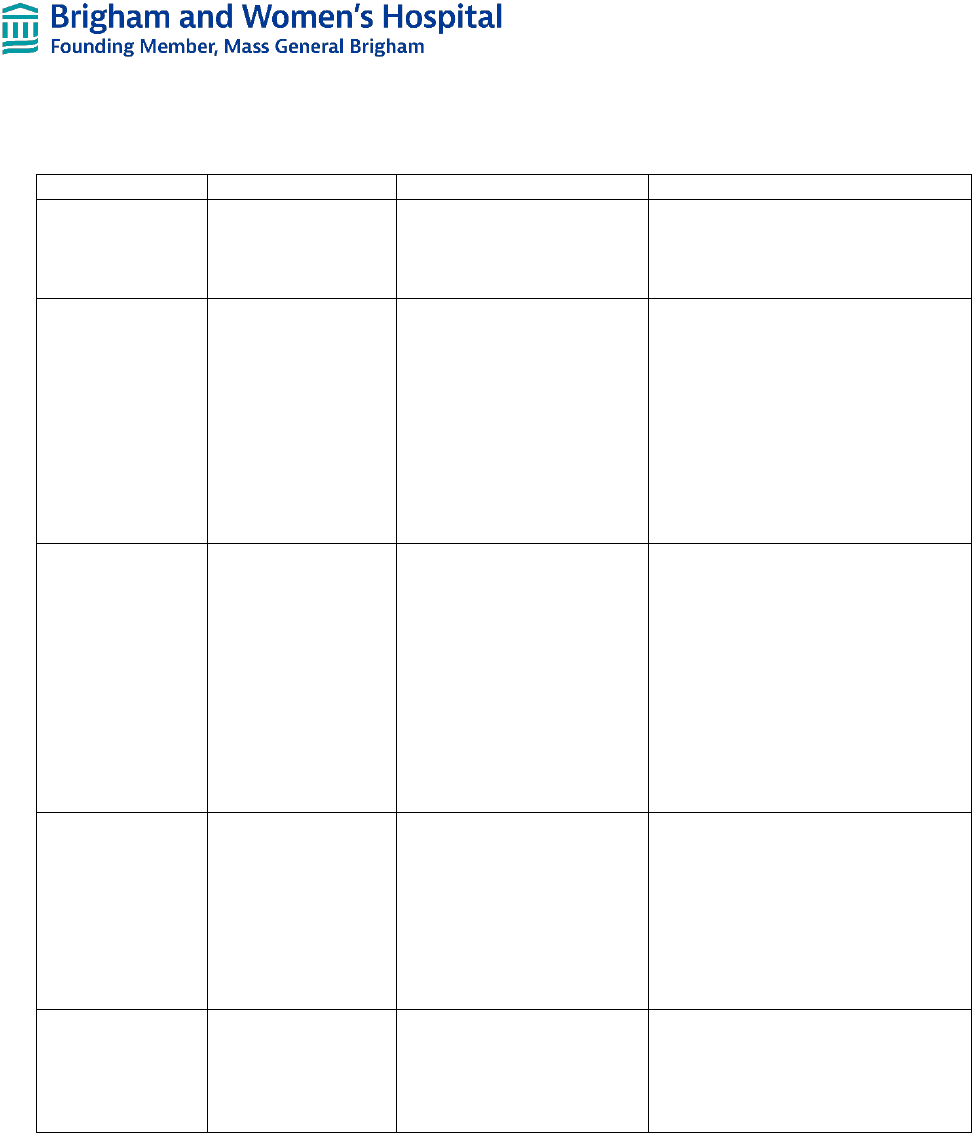
Progressive Resistive Exercises
• Biceps curls
• Triceps extensions
• Bent-over rows
• IR and ER in neutral with resistance
bands or in sidelying
• Progress to bilateral GH ER at or after
week 12
• HEP: to be completed 1-2x a day
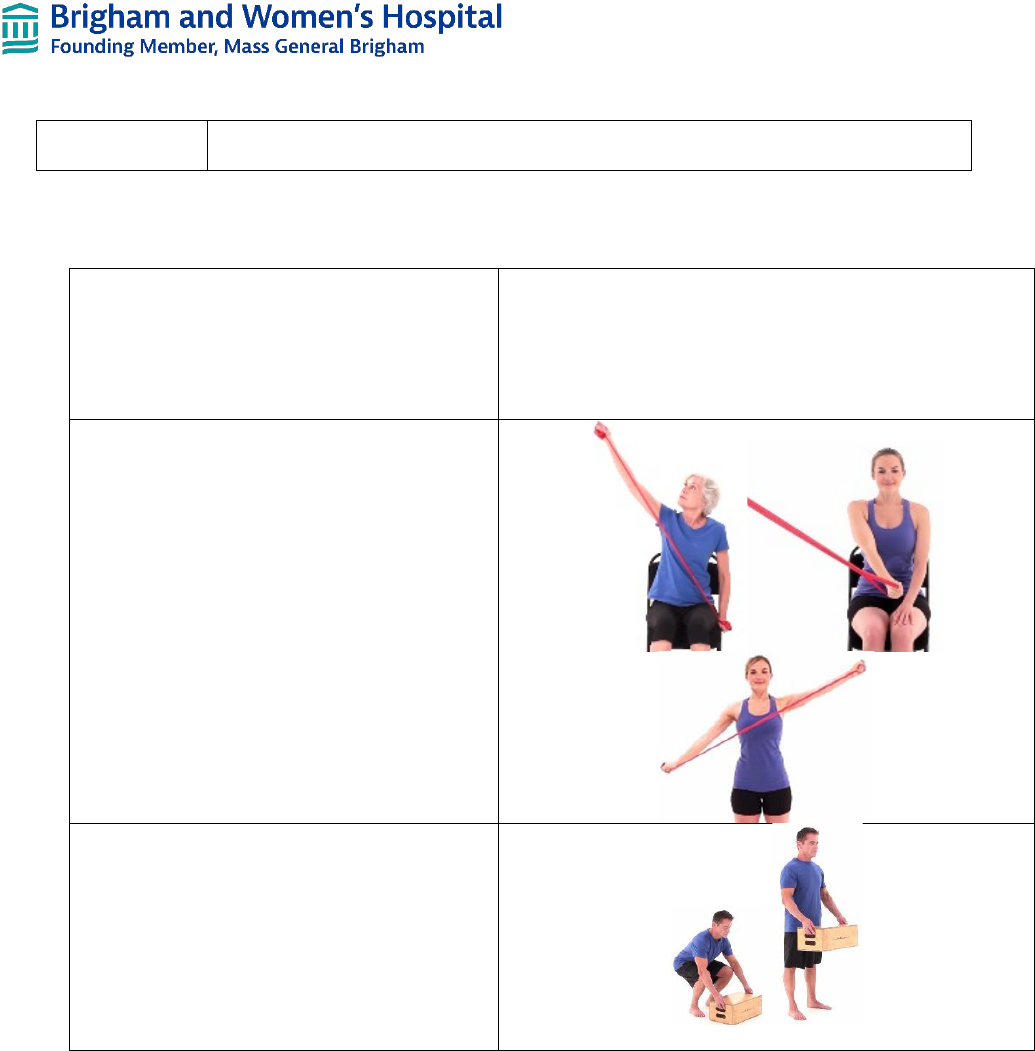
AAROM – Extension and behind the back cross
body adduction
• To be started at or after week 12
• In pain-free range of motion
• Focus on upright posture to avoid stress
on anterior shoulder structures
• HEP: to be complete 1-3x a day for short
hold (times 2-3 seconds)
Stretching – Shoulder IR Behind-the-Back with
Pulleys
• In pain-free ROM
• Focus on upright posture to avoid stress
on anterior shoulder structures
• 3x30 second holds
• HEP: to be completed 1-2x a day
Note: Add to program of those who have
achieved good shoulder extension and behind the
back cross adduction only; those with a limited
goal approach may not need to progress to this
exercise
Phase V – Return to Activity Phase (Weeks 16-24)
Goals
- Restore pain-free functional ROM
- Restore functional strength
- Progress weight bearing exercises as appropriate
Precautions
- Repetitive overhead lifting (communicate with surgeon for specifics)
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
13
Things to avoid
- Activities and exercises that stress the anterior capsule and subscapularis (i.e. combined
abduction and ER exercises, throwing motions, goal post pectoralis stretching, etc.)
Interventions:
Continue exercises and stretches from previous
stage
• Progress resistance band interventions
as appropriate
• Progress to weights as appropriate
Proprioceptive Neuromuscular Facilitation
patterns
• In pain-free ROM
• With resistance bands and/or weights
Sports/Work-specific training
• As needed
• Focusing on proper mechanics including
scapulohumeral rhythm
Criteria for discharge from skilled therapy:
• Independence and compliance with home exercise program to be continued 2-3x a week for continued
improvement in muscle strength and endurance
• Able to maintain pain-free AROM in multiple planes of motion
• Normal scapulohumeral rhythm with upper extremity elevation
• Maximized functional use of affect upper extremity
• Restored functional strength of upper extremity
• Returned to advanced functional activities

Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
14
FREQUENTLY ASKED QUESTIONS
1) How long should a patient wear a sling?
• A patient can start to wean from the sling between 6 and 10 weeks depending on past
medical history, intraoperative intervention performed, and surgeon recommendations
2) What are the positional precautions after a total shoulder arthroplasty if a subscapularis repair is
performed?
• External rotation especially in an abducted position
• Hyperextension as with sleeping without a sling or towel roll for support, particularly in the
early post-operative phases
3) What are the initial active movement precautions following a total shoulder arthroplasty if a subscapularis
repair is performed?
• Active internal rotation with ADLs such as tucking in shirt
• Weight-bearing activities such as with sit-to-stands and bed moblity
• Driving
• Lifting ADLs
• Any movements that put stress on anterior shoulder structures
4) How long are these precautions necessary?
• Depending on the surgery performed, 10-12 weeks depending on past medical history,
intraoperative intervention performed, and surgeon recommendations
5) When is it appropriate to begin AA/AROM?
• Approximately 6 weeks post-operative based on past medical history, intraoperative findings,
surgical intervention performed, and surgeon recommendations
6) Why are these limitations so important for these patients?
• Most of the precautions in these rehabilitation guidelines, especially in stage II, are to protect
the subscapularis tenodesis or less tuberosity osteotomy to allow for increased soft tissue
healing. Failure of the subscapularis repair can lead to increased pain, weakness, anterior
shoulder instability, early glenoid loosening, and reduced patient-reported outcomes.
Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
15
REHABILITATION PHASE SUMMARY CHART
Phase
Precautions
Goals
Interventions
Immediate Post-
Surgical
(Day 1)
- Sling use as
instructed
- No AROM or
weight bearing (WB)
- Understand activity
restriction and sling use
- Decreased pain and
inflammation
- Elbow, forearm, wrist, hand, finger
AROM
- Cryotherapy
Protection
(Day 2 - Week 6)
- Sling use
- Light, pain-free
ADLs only
- No AROM
especially IR, ER
PROM >20°
- No WB
- No lifting
- No driving
- Protect subscapularis
- Tissue healing
- Restore active elbow,
wrist, and hand movement
- Decrease muscle guarding
- Independence in light
ADLs
- 120° flexion PROM
- 15-20° ER PROM
- Minimal pain
- Flexion and ER PROM
- Scapulothoracic mobilizations
- Glenohumeral joint mobilizations
(Gr I-II for pain control)
- Cervical AROM and stretches
- Scapular retractions
- Pendulums
Intermediate
(Weeks 6-10)
- No painful or
strenuous ADLs
- No lifting more
than coffee mug
- No WB
- No reaching into
extension and IR
- No repetitive
active motions
- Protect subscapularis
- Scapular strengthening
- Optimize neuromuscular
control
- Weaning from sling
- Tolerate isometric muscle
activation
- 90° flexion AROM in
standing
- >140° flexion PROM
- 30° ER PROM
- Flexion, scaption, ER, and
abduction PROM
- Scapulothoracic mobilizations
- Glenohumeral joint mobilizations
(Gr III-IV for joint mobility)
- Flexion, ER, abduction, and
scaption AAROM
- Deltoid, IR, and ER isometrics
- Serratus anterior protraction
- Distal upper extremity
strengthening
Advanced
Strengthening
(Weeks 10-16)
- No repetitive
activities especially
against gravity
- No lifting >10#
- No heavy
pushing/pulling
- No sudden jerking
motions
- Protect subscapularis
- Increase AROM
- Return to functional
activities
- Increase strength
- 140° flexion AROM
- 160° flexion PROM
- 60° ER PROM
- AROM all planes
- Rhythmic stabilizations
- Postural strengthening
- WB exercises
- Stretching (behind the back and
across the chest)
- Progressive Resistive Exerises
Return to Activity
(Weeks 16-24)
- Repetitive
overhead lifting
- Stress on
subscapuaris
(throwing, etc.)
- Protect subscapularis
- Restore pain-free
functional ROM and
strength
- Progress to WB exercises
- Continue with strengthening
program
- Proprioceptive Neuromuscular
Facilitation
- Work/Sports-specific training
Is a BWH clinical competency associated with the document: Yes
Author Reviewers
Rachel Laufer, PT August 2022 Reg B. Wilcox III, PT August 2022
Stephanie Boudreau, PT August 2022

Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
16
References
1. Armstrong AD, Southam JD, Horne AH, Hollenbeak CS, Flemming DJ, Kothari MJ. Subscapularis function
after total shoulder arthroplasty: electromyography, ultrasound, and clinical correlation. J Shoulder Elbow
Surg. 2016;25(10):1674-1680.
2. Bornes TD, Rollins MD, Lapner PLC, Bouliane MJ. Subscapuarlis management in total shoulder
arthroplasty: current evidence comparing peel, osteotomy, and tenotomy. J Shoulder Elbow Arthroplasty.
2018;2:1-10.
3. Brown DD, Friedman RJ. Postoperative rehabilitation following total shoulder arthroplasty. Orthop Clin
North Am. 1998;29(3):535-547.
4. Eiter BE, Pehilvan HC, Brockmeier SF. Postoperative rehabilitation and outcomes of primary anatomic
shoulder arthroplasty. Tech Shoulder Elb Surg. 2016;17(1):19-24.
5. Koh KH, Lim TK, Shoon MS, Park YE, Lee SW, Yoo JC. Effect of immobilization without passive exercise
after rotator cuff repair. J Bone Joint Surg Am. 2014;96(6);(1-9).
6. Mulieri PJ, Holcomb JO, Dunning P, et al. Is a formal physical therapy program necessary after total
shoulder arthroplasty for osteoarthritis? J Shoulder Elbow Surg. 2010;19(4):570-579.
7. Papalia R, Franceschi F, Vasta S, Gllo A, Maffulli N, Denaro V. Shoulder stiffness and rotator cuff repair.
Brit Med Bull. 2012;104:163-174.
8. Postacchini R, Paoloni M, Carbone S, Fini M, Santilli V, Postacchini F, Mangone M. Kinematic analysis of
reaching movements of the upper limb after total or reverse shoulder arthroplasty. J Biomech.
2015;48(12):3192-3198.
1
Van Thiel GS, Wang VM, Wang FC, et al. Biomechanical similarities among subscapularis repairs after shoulder
arthroplasty. J Shoulder Elbow Surg. 2010;19(5):657-663.
2
Choate WS, Kwapisz A, Momaya AM, Hawkins RJ, Tokish JM. Outcomes for subscapularis management
techniques in shoulder arthroplasty: a systematic review. J Shoulder Elbow Surg. 2018;27(2):363-370.
3
Blacknall J, Bidwai AS. Rehabilitation following anatomic total shoulder replacement for osteoarthritis. NZ J
Physiother. 2020;48(2):80-91.
4
Bullock GS, Garrigues GE, Ledbetter L, Kennedy J. A systematic review of proposed rehabilitation guidelines
following anatomic and reverse shoulder arthroplasty. J Orthop Sports Phys Ther. 2019;49(5):337-346.
5
Wright T, Easley T, Bennett J, Struk A, Conrad B. Shoulder arthroplasty and its effect on strain in the subscapularis
muscle. Clin Biomech. 2015;30:373-376.
6
Singh JA, Sperling JW, Cofield RH. Revision surgery following total shoulder arthroplasty: analysis of 2588
shoulders over three decades (1976-2008). J Bone Joint Surg Br. 2011; 93(11):1513-1517.
7
Denard PJ, Lädermann A. Immediate versus delayed passive range of motion following total shoulder
arthroplasty. J Shoulder Elbow Surg. 2016; 25:1918-1924.
8
Keener JD, Galatz LM, Stobbs-Cucchi G, Patton R, Yamaguchi K. Rehabilitation following arthroscopic rotator cuff
repair: a prospective randomized trial of immobilization compared wit hearly motion. J Bone Joint Surg Am.
2014;96(1):11-19.
9
Keener JD, et al. 2014
10
Long JL, Ruberte Thiele RA, Skendzel JG, Jeon J, Hughes RE, Miller BS, Carpenter JE. Activation of the shoulder
musculature during pendulum exercises and light activities. J Orthop Sports Phys Ther. 2010;40(4):230-237.
11
Gaunt BW, McCluskey GM, Uhl TL. An electromyograhic elevation of subdividing active-assistive shoulder
elevation exercises. Sports Health. 2010;2(5):424-432.
12
Dockery ML, Wright TW, La Stayo PC. Electromyography of the shoulder: an analysis of passive modes of
exercise. Orthopedics. 1998;21(11):1181-1184.
13
Guerney AB, Mermier C, Laplante M, et al. Shoulder electromyography measurements during activities of daily
living and routine rehabilitation exercises. J Orthop Sports Phys Ther. 2016;46(5):375-383.

Department of Rehabilitation Services
Total Shoulder Arthroplasty Guideline
Copyright © 2022 The Brigham and Women's Hospital, Inc., Department of Rehabilitation Services. All rights reserved
17
14
Dockery ML, et al. 2018
15
Gaunt BW, et al 2010.
16
Muraki T, Aoki M, Uchiyama E, Takasaki H, Murakami G, Miyamoto S. A cadaveric study of strain on the
subscapularis muscle. Arch Phys Med Rehabil. 2007;88(7):941-946.
17
Guerney et al. 2016
18
Izquierdo R, Voloshin I, Edwards S, et al. Treatment of glenohumeral osteoarthritis. J Am Acad Orthop Surg.
2010;18(6):375-382.
19
Kirsh JM, Namdari S. Rehabilitation after anatomic and reverse total shoulder arthroplasty. J Bone Joint Surg Am.
2020;8(2):1-10.
20
Gaunt BW, et al. 2010
21
Cahill JB, Cavanaugh JT, Craig EV. Total shoulder arthroplasty rehabilitation. Tech Shoulder Elb Surg.
2014;15(1):13-17.
22
Blacknall J, et al. 2020.
