HE
1780
.A33
no.
91/03
WASHINGTON,
DC.
20594
RAILROAD ACCIDENT REPORT
ATCHISON, TOPEKA AND
SANTA FE RAILWAY COMPANY (ATSF)
FREIGHT TRAINS ATSF 818 AND ATSF 891
ON THE ATSF RAILWAY
CORONA, CALIFORNIA
NOVEMBER 7, 1990

n i- -
AW'
<3//o3
NTSB/RAR-91/03
PB91-916303
NATIONAL TRANSPORTATION
SAFETY
BOARD
WASHINGTON, D.C.
20594 !
i;
RAILROAD
ACCIDENT
REPORT
ATCHISON,
TOPEKA
AND
bANTA
FE
RAILWAY
COMPANY
(ATSF)
FREIGHT
TRAINS
ATSF
818 AND
ATSF
891
ON THE
ATSF
RAILWAY
CORONA,
CALIFORNIA
NOVEMBER
7
f
1990
ADOPTED:
July
23,1991
NOTATION:
5413A
Abstract:
This report explains the collision between two
Atchison,
Topeka and Santa
Fe
Railway freight trains in Corona, California, on November 7, 1990 Among the
safety
issues
discussed
are the following. effect of work/rest
cycles
on performance,
crashworthiness
of event recorders and locomotives, fuel tanks, positive train
separation,
company's method of detecting drug use by its employees, company's
method of notifying pipeline operators of accidents, need to develop simplified
format for work-record data collected by rail carriers, and need to develop policy
blocking employees from working if they lack sleep
The National Transportation Safety Board
is an
independent Federal agency
dedicated
to
promoting
aviation, railroad, highway, marine, pipeline,
and
hazardous materials safety Established
in 1967, the
agency
is
mandated
by the
Independent Safety Board
Act of 1974 to
investigate transportation accidents,
determine
the
probable cause
of
accidents, issue safety recommendations, study
transportation safety
issues,
and
evaluate
the
safety effectiveness
of
government
agencies
involved
in
transportation
The
Safety Board makes public
its
actions
and
decisions
through accident reports, safety studies, special investigation reports,
safety recommendations, and statistical reviews
Information
about available publications may
be
obtained
by
contacting:
National Transportation Safety Board
Public
Inquiries Section, RE-51
800
Independence Avenue, S.W.
Washington,
D.C.
20594
(202)382-6735
Safety
Board publications
may be
purchased,
by
individual copy
or by
subscription,
from:
National Technical
Information
Service
5285
Port Royal Road
Springfield, Virginia
22161
(703)487-4600
CONTENTS
EXECUTIVE
SUMMARY
INVESTIGATION
Accident }• ^
Injuries
Damages
Crew
Information
ATSF818
Engineer
Conductor
ATSF891
Engineer
Conductor
Train
Information
General
ATSF818
ATSF891
Track and Signal
Information
Track
Signal
Radio
Operational
Information
Work/Rest Cycles
Operations .. .
Meteorological
Information
Medical and Pathological
Information
ATSF
818
Engineer ...
Conductor
Brakeman
ATSF891
Engineer ...
Conductor
Brakeman
Injuries
Fatal •
Survivors
Toxicology for Drug Testing
Drug Policy
Fire
Postaccident Damage Examination — ...
Survival
Aspects •
Emergency Response
Crashworthiness
Pipeline
Information
Natural Gas Pipeline
Petroleum Pipeline
Tests and Research
Sight Distance .
Signal
System
iii
Event
Recorders 28
Natural Gas Pipeline 29
Petroleum Pipeline 29
Other
Information
29
Pipeline Notification 29
Locomotive Fuel Tank 29
Positive
Train Separation System 30
ANALYSIS
General 30
Accident 30
Work/Rest Cycles 31
Engineer of
train
818 31
Conductor of
train
818 35
Brakeman of
train
818 35
Behavioral Actions of the Crew of Train 818 36
Acceptance of Work Assignment 37
Positive
Train Separation 40
Pathological 41
Drug Issue 42
Conductor of
train
891 , 42
Engineer of
train
891 42
Work Records 43
Locomotive Crashworthiness 43
Fuel
Tank Crashworthiness 44
Event
Recorders • 44
Notification of Pipeline Operators 45
CONCLUSIONS
Findings 45
Probable Cause 46
RECOMMENDATIONS
46
APPENDIXES
Appendix A-lnvestigation and Hearing ... 49
Appendix B-Personnel
Data
51
Appendix C-Rules Applicable to this Report .. 53
Appendix
D-Notification
Form Used by
ATSF
for Pipeline Operators 55
Appendix
E--ATSF
Drug Policy 57
Appendix F-Track Map of Collision Site — . 65
iv
iXECUTIVE SUMMARY
On
Wednesday,
November 7, 1990, about 4 11am
Pacific
standard time, two
Atchison,
Topeka
and
Santa
Fe
Railway
Company
(ATSF)
freight
trains collided head
on at milepost
(MP)
25.6 in Corona, California. The westbound
ATSF
freight
train
818, which was traveling
from
Barstow, California, to Hobart yard, City of
Commerce,
California, was on the Corona siding It passed the stop signal, and the
lead
locomotive reentered the main track
area,
blocking all movement on the main
track The eastbound
ATSF
freight
train
891, which was traveling
from
Hobart yard
to
Chicago,
Illinois, was on the main track and collided
with
train
818.
Each
train
had
three-person crews
As
a result of the collision, the entire crew of
ATSF
818 was
killed
and
four
locomotives and three rail
cars
were derailed The engineer and conductor of
train
891 sustained serious injuries and the brakeman was killed, all three locomotives
and
five rail
cars
were derailed The
total
damage was estimated to be $4,400,000.
The
major safety
issues
addressed
in the report are
o
Effects of the
Crew's
Work/Rest
Cycle
on Performance
o
A Drug Policy Follow-Up
Issue
o
Crashworthiness of
Event
Recorders
in an Accident
The
National Transportation
Safety
Board determines that the probable
cause
of the collision was the failure of the engineer of
train
818 to stop his
train
at the
stop signal because he was asleep Contributing to the accident was the failure of
the conductor and the brakeman to take action, probably because they too were
asleep,
to stop the
train
Also
contributing
to the accident were the irregular
unpredictable work schedule of the engineer on
train
818, the Atchison, Topeka and
Santa
Fe
Railway
Company's lack of a policy or procedure for removing
crewmembers
from
service when they are not fit for duty because of a lack of sleep,
and
the inadequacy of the Federal rules and regulations that govern hours-of-
service
As
a result of its investigation, the
Safety
Board issued recommendations to the
Atchison,
Topeka and
Santa
Fe
Railway
Company, the Federal Railroad
Administration, the California Public Utilities Commission, the California
State
Fire
Marshal,
the Brotherhood of Locomotive Engineers, the United I ransportation
Union,
and the Association of American Railroads.
v
NATIONAL
TRANSPORTATION SAFETY BOARD
WASHINGTON, D.C.
20594
RAILROAD
ACCIDENT
REPORT
COLLISION
OF
ATCHISON, TOPEKA AND
SANTA
FE
RAILWAY COMPANY (ATSF)
FREIGHT
TRAINS ATSF
818 AND
ATSF 891 ON THE ATSF RAILWAY
CORONA, CALIFORNIA
NOVEMBER
7,1990
INVESTIGATION
Accident
On
November 6, 1990, at 10.15 p m.
Pacific
standard time, the crewmembers
on the Atchison, Topeka and
Santa
Fe
Railway
Company
(ATSF)
freight
train
818
went on
duty
at
their
away-from-home terminal in Barstow, California. Train 818
was
a westbound cabooseless
freight
train
originating
in Barstow and destined for
Hobart yard in the City of
Commerce,
California. The
train
consisted of 5 locomotives
and
91
rail
cars
(74 were loaded and 17 were empty) It had 8,616
trailing
tons and
was
5,996
feet long
Barstow
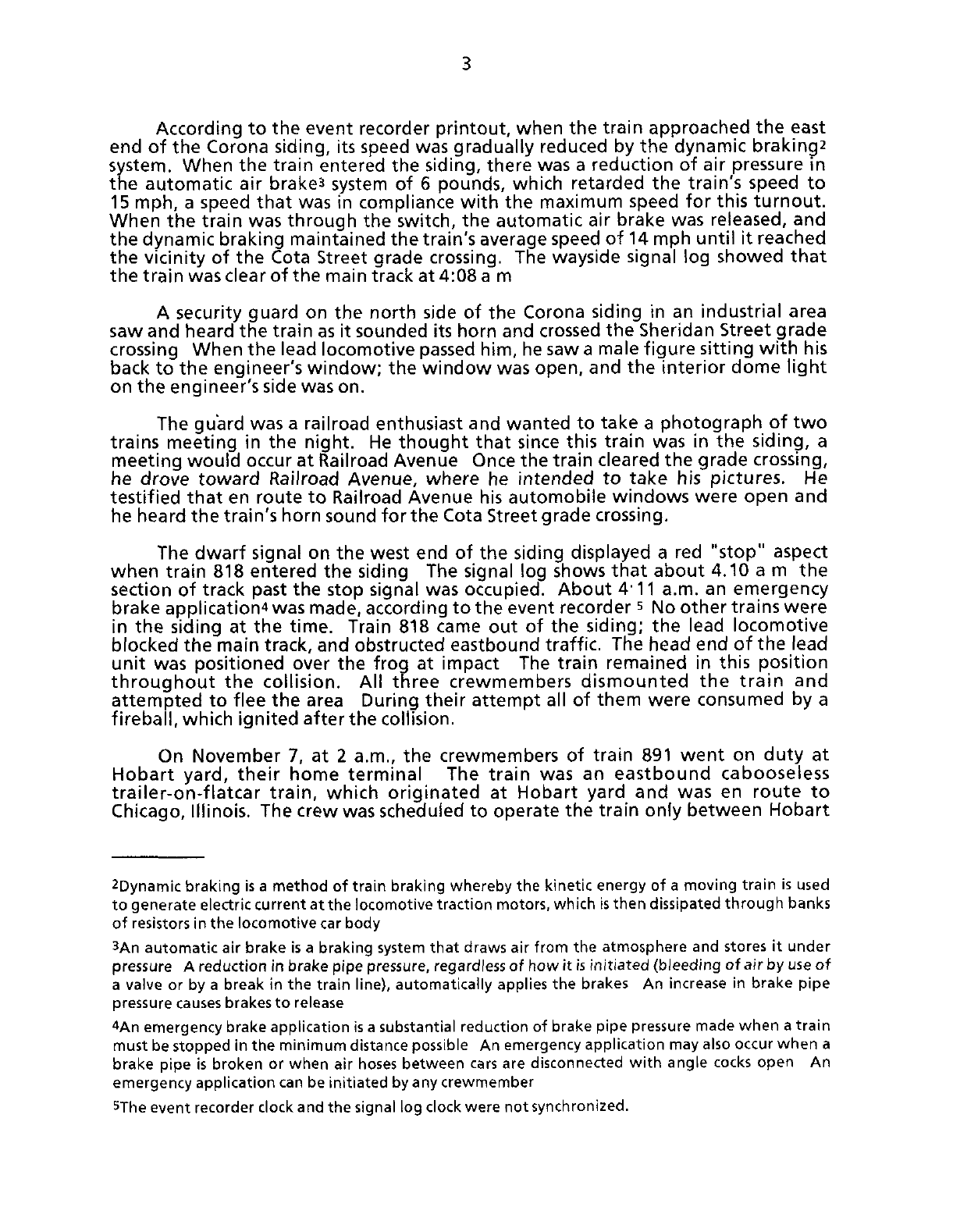
was part of the Cajon subdivision; Hobart yard was part of the San
Bernardino subdivision. Both subdivisions were part of the
ATSF
California division,
and,
as
figure
1
illustrates, the Cajon subdivision extended
from
Barstow to the city
of
San
Bernardino, and the
San
Bernardino subdivision extended
from
the city of the
same
name to Los Angeles. Both subdivisions were governed by centralized
traffic
control
(CTC)J
timetables, track warrants, and
train
orders.
The
crew of
train
818 consisted of an engineer, a conductor, and a brakeman,
all of whom, according to
ATSF
records, were qualified to operate in this
territory
The
brakeman was on the
return
portion
of her
first
road
trip.
All of the
crewmembers
had been off
duty
for 9 hours 35 minutes since
their
previous
tour
of
duty.
According to the event recorder
printout,
the
train
left
Barstow yard about
midnight.
It stopped
from
12 47 a.m. to 12*57 a.m so that a helper engine could be
coupled to its rear end. The helper engine was to stay
with
train
818
until
it arrived
at
San
Bernardino yard.
The
train
spent 4 minutes in
San
Bernardino so that the helper engine could be
uncoupled. During the stop, the assistant
train
master noted that the engineer
appeared
to be
tired
while he was in the yard office Other
ATSF
personnel saw the
brakeman dismount the engine
during
this time and stand alongside it After the
stop, the
train
continued west, via the San Bernardino subdivision, toward Hobart
yard According to the
ATSF
manager of operation's testimony, the
San
Bernardino
dispatcher
notified
the
train
about 3.52 a m. that it would be going
into
the siding
at Corona to meet an eastbound train.
1CTC
is a term applied to a system of railroad operations by means of which the movement of trains
over
routes and
through
blocks on a designated section of track or tracks is directed by signals
controlled
from
a designated central
point

LOS ANGELES
t J
MILES
—
HOBART VARD
3 5.!
MILES
—
PRADO DAM
5 J
MILES
—
CORONA
14 3
MILES
RIVERSIDE
».7
MII.ES
SAN BERNARDINO
_
IS.6
MILES
—
SUMMIT
-
6 3.4
MILES
—
BARSTOW
Map
of
the
Atchison,
Topeka
and
Santa
Fe
Railway
Main Track
System
From Los Angeles, California
To
Barstow
California
Barstow
MP 745.9
Enlarged Area
"3,
San
Bernardino
Subdivision
Los
Angeles
Starting Terminal'
for train 891
Starting terminal
for train 818
Pasadena
Branch
San
Bernardino
Distances
of
Grade Crossings from
the East Switch Of The Corona
Siding
•
Main Street 565 Feet
Sheridan Street 1,786 Feet
Cota Street 2,914 Feet
Railroad Avenue 8,272 Feet
Ah-
Collision Site
[]At Corona,
CA.
Industrial Siding
Four
Cwnrr3^^
Pipe Company
Petroleum
Lint
ATSF Main Track
Map Produced by
NTSB
Map Not
To
Scale
Figure
1
~
Map
of
the Atchison, Topeka and Santa Fe Railway
main track system
from
Los
Angeles
to
Barstow
3
According
to the event recorder printout, when the train approached the east
end of the Corona siding, its speed was gradually reduced by the dynamic braking
system.
When the train entered the siding, there was a reduction of air pressure in
the automatic air brake3 system of 6 pounds, which retarded the train's speed to
15 mph, a speed that was in compliance with the maximum speed for this turnout.
When
the train was through the switch, the automatic air brake was released, and
the dynamic braking maintained the train's average speed of 14 mph until it reached
the vicinity of the Cota Street grade
crossing.
The wayside signal log showed that
the train was clear of the main track at 4:08 a m
A
security guard on the north side of the Corona siding in an industrial area
saw
and heard the train as it sounded its horn and
crossed
the Sheridan Street grade
crossing
When the lead locomotive passed him, he saw a male figure sitting with his
back
to the engineer's window; the window was open, and the interior dome light
on
the engineer's side was on.
The guard was a railroad enthusiast and wanted to take a photograph of two
trains meeting in the night. He thought that since this train was in the siding, a
meeting would occur at Railroad Avenue Once the train cleared the grade
crossing,
he
drove toward Railroad Avenue, where he intended to take his pictures. He
testified that en route to Railroad Avenue his automobile windows were open and
he
heard the train's horn sound for the Cota Street grade
crossing.
The dwarf signal on the west end of the siding displayed a red "stop" aspect
when
train 818 entered the siding The signal log shows that about 4.10 a m the
section
of track past the stop signal was occupied. About 4-11 a.m. an emergency
brake application*
was
made, according to the event recorder
s
No other trains were
in the siding at the time. Train 818 came out of the siding; the lead locomotive
blocked the main track, and obstructed eastbound traffic. The head end of the lead
unit was positioned over the frog at impact The train remained in this position
throughout the collision. All three crewmembers dismounted the train and
attempted to flee the area During their attempt all of them were consumed by a
fireball, which ignited afterthe collision.
On
November 7, at 2 a.m., the crewmembers of train 891 went on duty at
Hobart
yard,
their home terminal The train was an eastbound cabooseless
trailer-on-flatcar train, which originated at Hobart yard and was en route to
Chicago,
Illinois. The crew was scheduled to operate the train only between Hobart
2Dynamic
braking
is a
method
of
train
braking
whereby the
kinetic
energy of a
moving
train
is used
to generate
electric
current
at the
locomotive
traction
motors,
which
is
then
dissipated
through
banks
of
resistors
in the
locomotive
car
body
3An
automatic
air
brake
is a
braking
system
that
draws air
from
the
atmosphere
and
stores
it
under
pressure A
reduction
in
brake
pipe
pressure, regardless of how it is
initiated
(bleeding
of air by use of
a
valve or by a
break
in the
train
line),
automatically
applies
the brakes An increase in
brake
pipe
pressure causes brakes to release
4An emergency
brake
application
is a
substantial
reduction
of
brake
pipe
pressure made when a
train
must
be
stopped
in the
minimum
distance
possible
An emergency
application
may also occur when a
brake
pipe
is
broken
or when air hoses between cars are
disconnected
with
angle cocks
open
An
emergency
application
can be
initiated
by any
crewmember
5The event
recorder
clock
and the
signal
log
clock
were not
synchronized.
4
yard and Barstow. The train had 3 locomotives and 47 rail
cars
(all loaded). It
weighed 3,150 trailing tons and
was4,229
feet long.
The crew of train 891 consisted of an engineer, a conductor, and a brakeman,
according to
ATSF
records, all were qualified to operate in this territory.
The engineer of train 891 talked with Safety
Board
investigators after the
accident but refused to speak to the Safety
Board
during deposition proceedings In
his
testimony the conductor took no exception to the engineer's handling of the
train during theirtourof duty.
The conductor stated that he and the engineer were in the lead (eastmost)
controlling locomotive and that the brakeman was in the second locomotive. The
brakeman, according to the conductor's testimony, chose of his own volition to ride
in the second unit.
The conductor further stated that as the train approached Corona, the CTC
signals
were displaying aspects^ permitting it to proceed eastward When the train
reached signal 2R (located at the west end of the Corona siding and governing
eastbound traffic on the main track), the aspect changed from a yellow "approach"
indication to a green "clear" indication. The yellow indication allowed train 891 to
proceed but required that it be prepared to stop at the next signal and restricted the
train speed to 40 mph. The clear indication allowed the train to proceed at the
maximum authorized speed.
The conductor stated that when he saw the "clear" signal, the overhead
speedometer on the
left
side of the cab, where he was seated, indicated that the
train was traveling about 29 mph
He testified that when the train was about four or five car lengths from the
signal,
he got up from his seat to get something from his bag. A moment later he
heard the engineer shout that the signal had changed The conductor said that the
"clear" aspect had changed to a red "stop" aspect and he saw the headlight of an
oncoming locomotive. He dropped to the floor and braced for the ensuing collision
The impact threw the crewmembers about within the confines of their respective
engine compartments. The engineer and the conductor sustained serious injuries,
and the brakeman was killed.
The
left
front corner end sill area of the lead locomotive unit of train 818
collided with the
left
front corner end sill area of the lead locomotive unit of
train 891; train 891's lead unit swerved to the south of the main track and landed on
its right side. The second locomotive unit landed on its
left
side along the north side
of the track The third locomotive unit proceeded eastward, ramping over parts
from the other two locomotives, and landed on top of the control cab of the lead
locomotive of train 818. An intense fire ensued.
About 4:24 a.m the
ATSF
dispatcher was notified by the Corona police
department that there was a railroad accident in the vicinity of Railroad Avenue and
Smith
Street. The dispatcher's office then notified those individuals listed on the
ATSF
emergency response form.
6An
aspect
is the
appearance
of a
fixed
signal
conveying
an
indication
5
Injuries?
Crew
of
ATSF
818 Crew of
ATSF
891 Total
Fatal
3 1 4
Serious
0 2 2
Minor 0 0 0
Total 3 3 6
Damages
The
ATSF
estimated damages
Equipment
$3,868,780
Track
50,000
Signal
35,000
Labor
10,052
Lading
Damage
450,000
Other (Railroad Property
Costs)
19,170
Total
$4,433,002
Crew Information
ATSF
818
Engineer.-On
Sunday, November 4, he worked a train from Barstow to Hobart
yard,
starting at 6:45 p m. and ending on November 5 at 7:30 a.m. He then drove
home, arriving just before 9 a.m. He went on a school field
trip
with his children,
returned home in the early afternoon, and took a short nap. After his nap, he
telephoned the
ATSF
Voice Information Processing System
(VIPS)
s
Following the
call,
he told his wife he expected to be called to work about 5 p.m. on the following
day,
November 6. He ate dinner with
his
family and went back to bed about 8 p.m.
About 1 30 a m on November 6, 1990, the wife of the engineer of train 818
received
a call from the
ATSF
crew caller^ who said her husband was to report for
work at 430 a m at Hobart yard. She woke her husband, and he
left
for Hobart
yard,
which was more than 60 miles away Before leaving, he told his wife that if he
arrived at Barstow before noon he would return home (San Bernardino) to take care
of one of their children while she attended her college
classes.
(He coowned an
automobile that was garaged in Barstow and would have used the car to travel back
to his house.) He reported at Hobart yard at 4:30 a.m and arrived in Barstow at
?The
injury
table
is
based
on
injury
criteria
used
by the
International
Civil
Aviation
Organization
(ICAO) The Safety Board uses
these
criteria
in all of its
reports.
8VIPS
is a
telephone/computer
interface
system
that
allows
ATSF
employees
to
obtain
the
current
train
line-up
and
their
own
work
status
relative
to
other
employees
in the same
pool
9The
crew
caller
gave
crewmembers
whose
home
terminal
was
Hobart
yard
as
much
as 3
hours
notice
before
they
were
to
report
for
duty
6
12:40 p m., too late to accommodate his wife He called from Barstow and told her
that since he anticipated a long layover, he did not expect to be called until the
following morning and was not going to bed until later that day
Accompanied
by the conductor and the brakeman, he checked into the
ATSF-contracted
motel at 1:30 p m. and went with them to eat. According to other
ATSF
personnel, he and the brakeman were in the recreation room of the motel
between 3:30 p.m and 6 p.m. About 6 p.m. they joined another engineer for
dinner, and they returned to the motel about 8 pm.
While
he was in Barstow, he talked to several other
ATSF
crewmembers who
were
waiting to be assigned to outbound trains Through them he became aware of
the status of the train line-up.
He
called the
ATSF
crew caller about 8:40 p.m. and learned that he was being
assigned
to a crew with a starting time of 10:15 p.m At that time he discovered that
three crews that were ahead of him in the line-up had been deadheaded.
10
During
his
conversation with the crew caller, he discussed the deadheading of the other
crews
and threatened to lay off" sick, implying that he had not slept Finally, he said
that he wanted to speak to the supervisor of train operations
(STO).
The crew caller
asked
him if he was going to accept the assignment; he replied,
"Well,
I got, I mean
what else am I going to do
...?"
During a
12-minute
recorded telephone conversation with the STO, the
engineer complained about the method of determining how trains were assigned
and,
particularly, about the deadheading of crews He told the
STO,"
.. I mean how
do you plan your life, you just live by
surprises?"
The
STO
testified that he concluded
from the conversation that the engineer had not been to bed while he was in
Barstow
He further testified that he was sympathetic to the engineer's situation At
the end of the conversation, the engineer did not lay off, he chose to accept the
assignment.
The
ATSF
regional manager testified that had the engineer asked to lay off, the
request would have been granted Although it was unusual for an employee to lay
off at an away-from-home terminal, the
ATSF
was aware that at times things
happened,
such as illness or family emergencies, that forced an employee to lay off
at an away-from-home terminal The regional manager further testified that crews
". normally would leave as a unit after they arrived as a unit"
The regional manager
said,
" . had he [the engineer] laid off, and he didn't
have
a history of it, and even though if it wasn't perceived as a good reason, I'm
confident there wouldn't have been any punitive measures taken, other than to say,
hey,
you need to get your act cleaned up . ."
10
Deadheading
is
off-duty
travel
when
train
crewmembers
are
moved
without
service but
with
pay
from
one
terminal
to
another
at the
railroad's
convenience
1
laying
off is a
method
by
which
an
employee
can
report
himself
not
available
for
duty
7
After he arrived at the Barstow terminal building, the engineer called his wife
at 10'15 p.m. to tell her that he was returning. She later told investigators that
during the telephone conversation he admitted that he was exhausted, that he had
taken only a small nap, and that he wanted to lay off. When she asked him why he
did not layoff, he replied, "I can't," and gave no further explanation
Investigators could not account for his actions between 8"55 p.m and 10 p.m.
When
the accident occurred, he had been awake for 26 hours 41 minutes, excluding
the brief period of rest in Barstow
Conductor --On November 4, the conductor was called at 9 a m. to work on a
train that was to leave Hobart at 12:01 p.m. and arrive at Barstow at 6.45 p.m. On
the following morning, November 5, he was called at 1:30 a.m. to take a return train
to Hobart that
left
at 2.45 a.m. and arrived at
10:15a.m.
He went home, and at
approximately 1:30 a.m. on November 6, he received his next
call,
which was again
to work a tr,ain from Hobart yard to Barstow.
As
had the engineer, the conductor reported at Hobart yard for a
trip
that
started at 4:30 a.m. on Tuesday, November 6 At 12:40 p m., he arrived at Barstow
yard.
He called his wife and told her that he would probably not get a return train
until about 5 a.m. the following day and that he was going to bed.
After eating with his crew, he returned to the motel and went to his room.
Investigators could not account for his actions between 230 p m. and 8 45 p.m ,
when the crew caller told him that he was assigned to train 818 The conversation
between him and the crew caller was recorded; the conductor sounded as if he had
just been awakened. When the accident occurred, he had been awake for
approximately 6 hours.
Brakeman-At 1:30 a.m. on November 6, the crew caller told the brakeman
that she was to go on duty at 4 30 a m. at Hobart yard. The
trip
was her first
interterminal tour as a brakeman. She
left
her house at 2.30 a.m and arrived at
Hobart yard about 3am
At Barstow, she joined the crew for a meal. When the crew returned to the
motel, she remained in the engineer's company until shortly after 8 p.m , when she
went to her room. The
ATSF
crew caller reached her at 8.43 p.m. and assigned her to
train 818. Her conversation with the crew caller was taped, and she sounded as if she
had just been awakened.
She
was next seen at
San
Bernardino yard, where the train
stopped for a 4-minute layover and she dismounted the engine. When the accident
occurred,
she had been awake for 26 hours 41 minutes, excluding the brief period of
rest in Barstow. Her activities on November 6 between 8 p.m and 10 p m. were
unknown
ATSF891
Engineer.-On Tuesday, November 6, at 11.15 p.m , the
ATSF
crew caller
reached the engineer and assigned him to train 891, which was to originate in
Hobart yard at 2 a.m. on Wednesday, November 7, and go to Barstow. He arrived at
Hobart yard about 1:30 a.m. and
left
about 3.10 a m. He had been off duty 25 hours
45 minutes before reporting to Hobart yard. He had been awake for 4 hours 56
minutes at the time of the collision and stated (during a postaccident interview with
investigators) that he had slept for most of the day and evening on Tuesday until he
was
awakened by the crew caller.
8
Conductor --On November 6, the conductor received a call from the
ATSF
crew
caller at 11' 15 p m , assigning him to train 891 En route to Hobart yard, he picked
up his brakeman for train 891; the two reported to Hobart yard about 2 a.m and
left
about 3:10 a.m. The conductor testified that he was in the controlling compartment
of the lead locomotive He had been off duty for 28 hours 20 minutes before
reporting to work. At the time of the accident, he had been awake for 6 hours
11 minutes
Brakeman
-He received his call assigning him to train 891 about 11:15 p.m. on
November 6. According to the conductor, the brakeman boarded the second
locomotive of his own volition. Before boarding the train, he had been off duty for
28 hours 20 minutes He had been awake 5 hours 11 minutes at the time of the
accident
Train Information
General -The
ATSF
assistant chief mechanical officer testified that
ATSF
locomotives had been equipped with alertersiz until about 10 years earlier. Due to
mechanical difficulties and lost production time, the
ATSF
had removed them. The
ATSF
did not use cab
signals^
in locomotives.
The assistant chief mechanical officer stated that the
ATSF
had a policy of
installing event recorders on even-numbered locomotives Investigators found that
in the fleet of about 1,800 locomotives, 65 odd-numbered units also were equipped
with event recorders. The officer said that the
ATSF
attempted to have an event
recorder on "97 percent" of its engine
consists
that were in road
service.
ATSF
818.-Train
818 consisted of 5 locomotives and 91 rail
cars
The
locomotive consist included
ATSF
5363
(Electro Motor Division
EMD-SD
45),
ATSF
5267
(EMD-SD
40-2),
ATSF
5395
(EMD-SD
45),
ATSF
8063
(General Electric-C
30-7),
and
ATSF
5328
(EMD-SD
45). Of the five locomotives units, only the
fifth
had an
event recorder.
The SD 45 locomotive had 11-gauge (or 0 125) mild steel in its nose section The
collision posts on the SD-45 were 59 inches high on the
left
and 54 inches high on the
right.
Both
posts were made of mild steel with a specified minimum yield strength
of
27,000
pounds per square inch (psi) See figure 2 for a photograph of an SD-45
locomotive.
The control compartment of the SD-45 was a standard design that had been
used
in the railroad industry since the early
1960s
The control compartment was
configured with the engineer's position on the right side and with the control stand
on the engineer's left. Two fully adjustable seats were on the
left
side wall, one
forward and one aft, forthe conductor and brakeman
i2An
alerter
is a
device
that
monitors
the
engineer
for
activity
and
provides
a
visible
and
audible
warning
for a
predetermined
length
of
time
after
which
a
penalty
air
brake
application
is
made
if the
system
is not
reset
13A
cab
signal
is a
device
in the
control
cab of the
locomotive
that
indicates
the
condition
of the
track
ahead
(clear
or
occupied)
by
displaying
lighted
signals

9
Figure
2.--SD-45
locomotive.
Top: General Motors Electro-Motive Division.
Bottom:
Engineer's control stand.
10
The SD-45 was equipped with
a
two-piece center horizontal windshield
and a
right
front
vertical windshield
Each
side
of the
control compartment
had two
operable slide-type side windows. One rear
fixed
vertical observation window was
at the
left
rear
of
the control compartment.
The
maximum
capacity
of the
fuel tanks
on the
SD-45 locomotive
was
4,000
gallons
of
diesel fuel. The end sill was
66
inches from the
top of
the rail
to the
top
of
the sill
Six
rail
cars
in the
train's consist contained hazardous materials. None
of
these
cars
was involved in the collision.
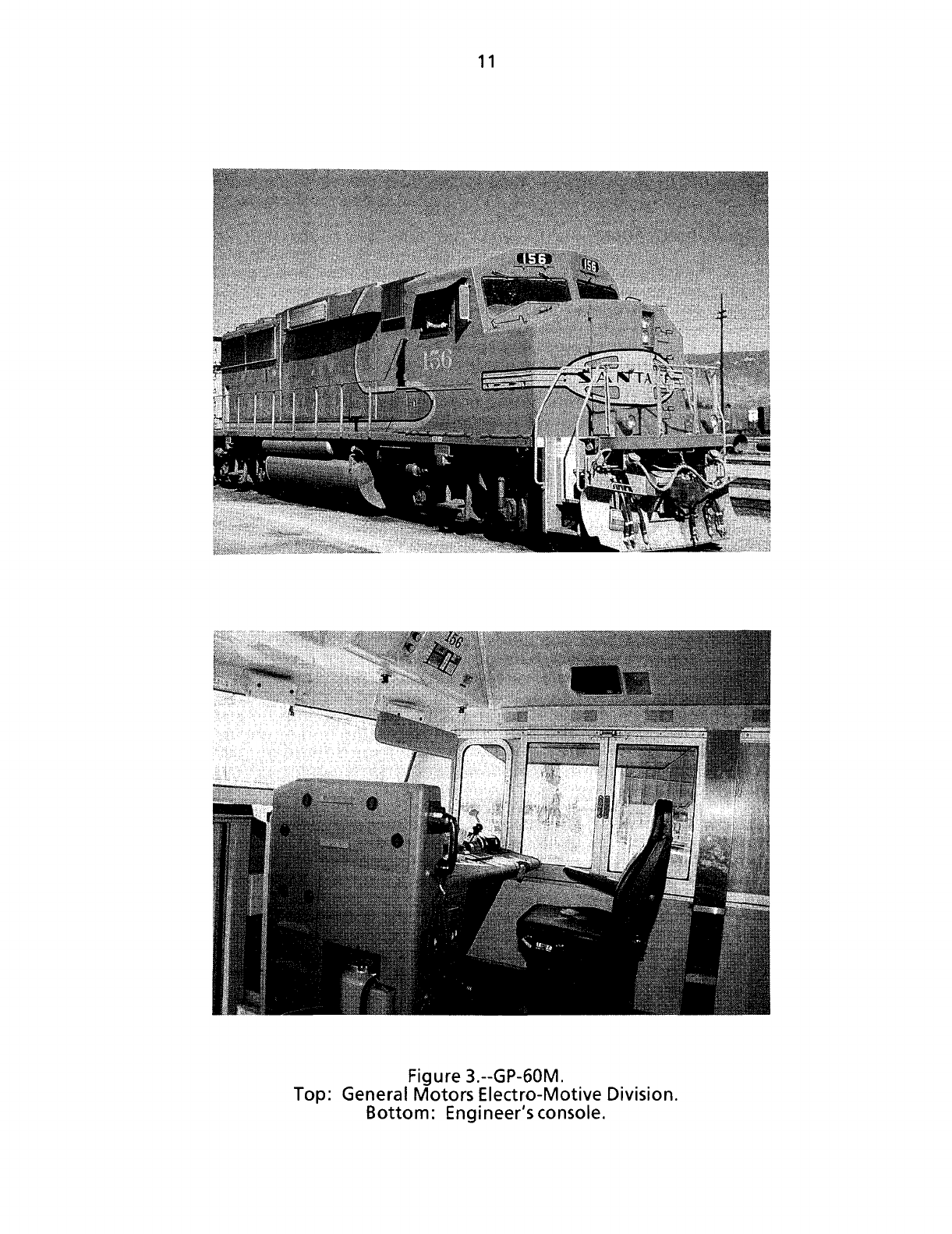
ATSF
891-Train
891's
locomotive consist
had
ATSF
137
(EMD-GP
60M),
ATSF
147
(EMD-GP
60M), and
ATSF
152
(EMD-GP
60M). The control compartments
of the
first and second locomotives faced east, while
the
control compartment
of the
third
locomotive faced west. Figure
3
is
a
photograph
of a
GP-60M locomotive. The train
had
47
rail
cars,
all of
which were
flat
cars
carrying either highway trailers
or
containers.
The second
and
third locomotives each
had an
experimental event recorder
that
was being tested
by the
ATSF
The
recorders were
in the
vestibule area
of the
control compartments
and
employed solid state recording media
to
record
the
events
instead
of
a removable magnetic tape cartridge.
The GP-60M featured
0
375-inch
high-strength steel
in its
nose section
and a
58.87-inch
high collision post
on
each side
of the
hood.
Both
collision posts were
made
of
high-strength steel
that
had
a
maximum
yield strength
of 50,000
psi.
All
the
locomotives were equipped with
a
North American-style control
compartment designed
in
part
by the
ATSF.
The new
control compartment
was
equipped with
a
desk
top
control console
on the
right,
or
engineer's, side.
On the
left
side were
two
fully adjustable
seats,
one
behind
the
other,
for the
conductor
and the brakeman. The design was based upon a design introduced
in
Canada in
the
early
1970s.
The North American control compartments were first introduced on
the
ATSF
in May 1990.
This was
the
first accident investigated
by the
Safety
Board
involving this type
of
control compartment.
At the
time
of the
report,
the
Federal
Railroad
Administration (FRA)
had no
data about
the
crashworthiness
of
North
American control compartments on locomotives
that
have been in collisions.
The forward entrance
of the
GP-60M was
a
heavy metal windowless door
on
the right side
of
the
front
wall. The exterior door led
to a
small vestibule in which
an
interior door led up two steps
to
the control compartment. The rear-entrance door,
which
had a
fixed
upper vertical window,
was at the
right rear
of the
control
compartment,
or
behind
the
engineer's seat.
The
door
led out to the
right-side
walkway, which ran alongside the engine compartment Figure
3
also illustrates
the
interior
of
the GP-60M control compartment.
The control compartment
had a
two-piece windshield,
two
operable sliding
side
windows (one on each side), and a
fixed
left-rear window. The rear wall had
an
electrical cabinet..
Each
unit
had a
fuel tank
that
could hold
3,200
gallons
of
diesel fuel
but
according
to
ATSF
policy, was limited
to 2,900
gallons
in
order
to
reduce
the
wear
and tear inflicted
on the
track
and the
locomotive's wheels.
The
locomotives
on
11
Figure 3.--GP-60M.
Top: General Motors Electro-Motive Division.
Bottom: Engineer's console.
12
train 891 had fast been fueled in
Belen,
New Mexico, on November 5; they
left
Hobart yard with approximately 1,000 gallons
each.
The sill height of the GP-60M was 63 inches from the top of the rail to the top
of the
sill.
Track and Signal Information
Track --At the collision point there was a single main track and a parallel siding,
both extending east to west The collision point was directly west of the Railroad
Avenue
grade crossing in the vicinity of the turnout
that
connected the single main
track and the west end of the Corona siding
(See
figure 1.) The accident occurred in
a light industrial area of warehouses and small shops Working street lamps flanked
and lit the north and south sides of the grade crossing
The track entering the Corona siding from the east had a descending gradient
of 0.47 percent for 1,306 feet. The track gradient continued to descend at
0.82 percent for 1,400 feet, at which point it became level. It was level for
2,685
feet
and then ascended at a gradient of 0 44 percent for
2,250
feet At
that
point, the
track gradient ascended 0.08 percent for 866 feet until it reached the west siding
turnout near Railroad Avenue
The main track extended east to west. The alignment at the collision point was
tangent. The main track was tangent for 8,184 feet from signal 272 to signal 2R and
continued to be tangent for another 40 feet past signal 2Rto the collision point. The
gradient at the collision point was descending at 0 08 percent
According
to the
ATSF
assistant superintendent of maintenance, the main track
was
maintained to
class
4 track standards^ at the Railroad Avenue grade crossing
The last time the track was inspected before the accident was on November 5 by an
ATSF
track inspector, and no defects were noted or reported
Siqnal.-The
signal system consisted of a traffic control system for a single-track
railroad having Union Switch and Signal Company
(US&S)
H-5 searchlight-type
signals
and a
US&S
M22A
dual-control switch machine. Noncoded track and line
circuits
were controlled from a
US&S
computer-aided dispatching center in San
Bernardino
The 2LB dwarf signal at the west end of the siding governed westbound traffic;
it was located near Railroad Avenue and displayed a "stop" indication when
train 818 entered the siding. According to the signal log, at 11 seconds past
4 10 a.m , the track circuit on the siding west of the
2LB
signal was occupied
Signal
2R, which was west of the west end of the Corona siding and along the
south side of the main track, was a home signal governing eastbound traffic.
According
to the signal log, at 8
seconds
past 4.09 a m , it displayed a "clear" aspect;
and at 11 seconds past 4-10 a m , it showed a red "stop" aspect, signifying
that
the
track circuit east of the signal was occupied
14
According
to 49 CFR
213.9,
class 4
track
is a
segment
of
track
maintained
to
accommodate
the
maximum
allowable
speed
of 80 mph for
passenger
trains
and the
maximum
allowable
speed
of 60
mph for
freighttrains
13
The Railroad Avenue grade
crossing
was protected by wig-wag warning signals
on
a mast alongside the roadway A round disc with a red lens lamp in its center
hung from the mast. When the crossing warning signal was activated, a bell rang
and the
disc
swung from side to side.
Radio
-The existence of recorded conversations between the dispatcher and
both crews shows
that
each train had an operational radio on board its respective
control locomotive. The
ATSF's
single radio frequency was used for "point to train"
communication, or communication by locomotive radio between the traincrew and
the dispatcher. The frequency was also used for "end to end" communication, or
communication by hand-held portable radio between the conductor and the rest of
the traincrew The dispatchers were in
San
Bernardino.
Operational
Information
Work/Rest
Cycles.-ATSF
operating employees used their seniority to place
themselves
in available work positions. The positions were in freight pool
service,
in
yard
service,
on routinely operated local trains, or on an
extra
board.is Employees
assigned
to yard and local train service had schedules
that
were generally based on
preestablished starting times.
The Safety
Board
obtained a list of the duty times for the engineer of train 818
during the
90-day
period (August 8 to November 6) before the accident. On
August
8,9, and 10, he worked in pool
service.
On August 11, he laid off on personal
leave
before beginning a vacation
that
lasted 22
days,
from August 12 until
September 2.
He
notified the carrier
that
he was available for service at 12'01 a m on
September 3 He got his first train on September 5 and remained in pool service
through September 16. On September 17, he transferred to the
extra
board and
remained on it through October 7, when he transferred back to pool
service.
From
October 7 until November 6, he worked nearly every time the pool rotation made
work available.
In the 64 days from September 5 through November 7, he worked 47 calendar
days
His tours included 3 in yard service and 53 in road
service;^
of the 56 tours, 7
were
deadheaded. On seven
occasions,
he had two tours of duty
that
started on the
same
calendar day.
(See
figure 4)
He
laid off
1
day on personal leave, 2 days
sick,
and 2 days while on
calM?
at his
home terminal. The carrier did not discipline him either time for marking off while
on
call.
Investigators noted
that
his average time on duty when he operated a train
was
7 hours 18 minutes. His average deadhead time was 2 hours 41 minutes. His
off-duty time between trips at his home terminal ranged from 11 hours 45 minutes
to 96 hours, the average time was 33 hours 12 minutes. His off-duty time at his
away-from-home terminal ranged from 2 to 27 hours; the average was 11 hours
15
Extra
board
engineers
fill
in
temporary
vacancies
created
when
other
employees
lay off for any
reason
These
vacancies
occur
in
freight
pools,
yard
service,
and
local
trains
15
Road
service
is the
movement
of
freight
over
the
railroad
from
one
terminal
to
another.
!7An
employee
is
considered
to be on
call
24
hours
a day If he
lays
off--says
he
cannot
work-without
giving
the
carrier
8
hours
notice,
he is
said
to be
"laying
off on
call
"

Chart
Of
The
Reporting Times
For The
Engineer
On ATSF 818
From
September
1,1990
Through
November 6,1990.
Last Day Worked
2400
2200
-h
2000
T
1800
w
1600
E
H
w>
1400
.5
§,
1200
v
Pi
iooo
• ;
osoo
-
\
0600
- •
0400
- ;
0200
T
0001
•
•
•
•
•
j_»
1111111111111111111 i 111111;
11111111
i f 11 1111 • 11111 • 111 • i 11 111 {1111
1-Sep
6-Sep
11-Sep 16-Sep 21-Sep 26-Sep
Source: ATSF Files
1-Oct
6-Oct
11-Oct 16-Oct
Dates Called
For
Work
21-Oct 26-Oct 31-Oct
Chart By NTSB
6-Nov
5-Nov
10-No
Figure
4.-- Reporting times for the engineer of train
818
from
September through November 1990.

15
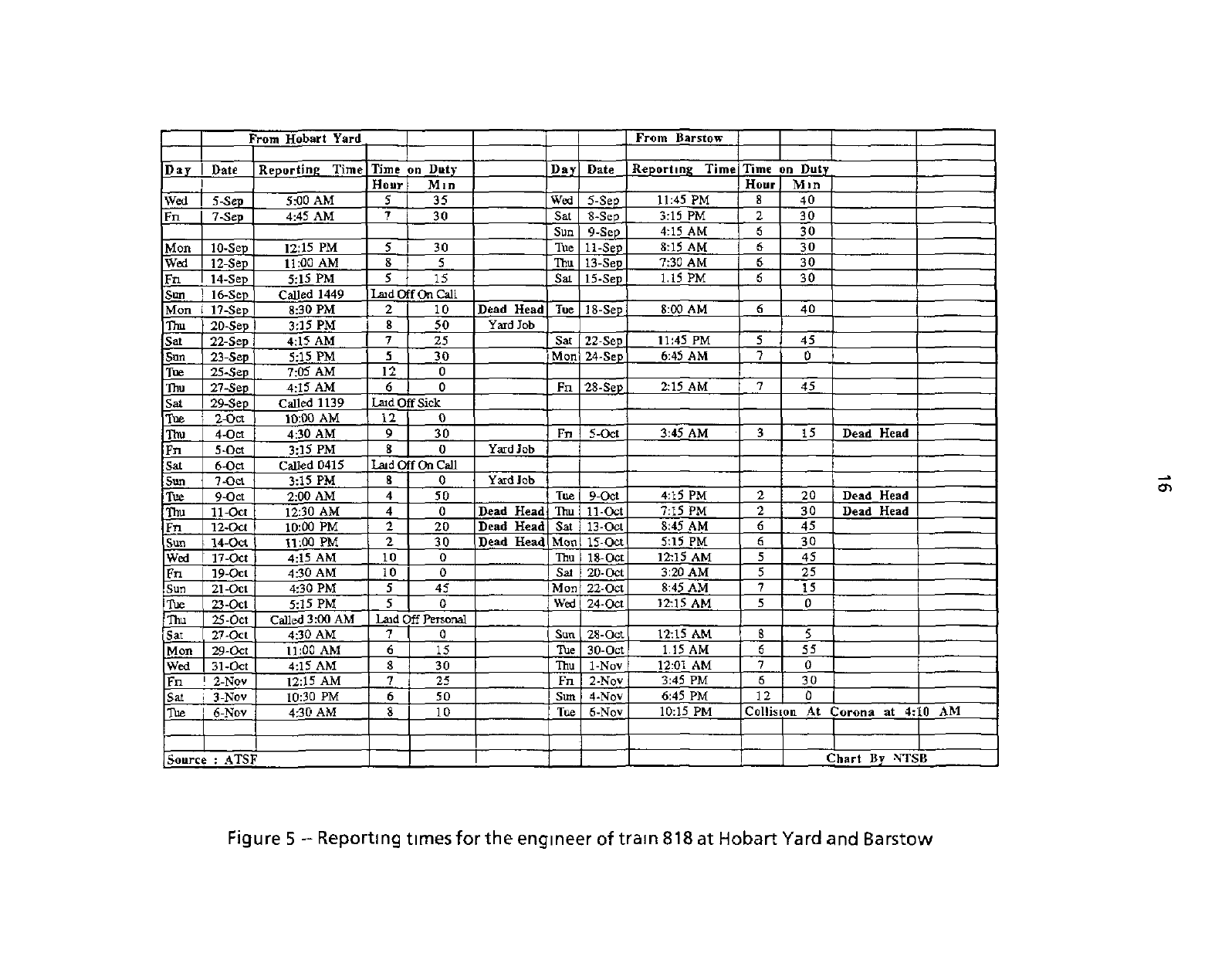
33 minutes Figure 5 shows the engineer's reporting times at both Hobart and
Barstow
yards.
Figure
4 illustrates the variation in his reporting time during the 64
days
before
the accident On April
1,1989,
Hobart yard became the home terminal for operating
personnel,
including the engineer of train 818, whose home terminal had been San
Bernardino
He continued to live in the San Bernardino area; his commuting time
increased
from 10 or 15 minutes to, depending on the traffic,
1
1/2 to 2 1/2 hours.is
When
he was in Barstow, he stayed at an ATSF-contracted motel about
5
minutes away from the terminal. He received his
calls,
on the average,
1
hour 5 minutes before his reporting time.
Operations.--The
ATSF
is among the 41 railroads that are signatories of the
General
Code of Operating
Rules.
(See appendix C for a listing of the rules referred
to in this report that are in the General Code )
At
San Bernardino, the main track split into the San Bernardino and Pasadena
subdivisions,
which were reunited at
Los
Angeles.
The
ATSF
manager of operations
(MOP)
testified that an average of 18 to 20 freight trains and 2 Amtrak passenger
trains traveled through the Corona station area in a
24-hour
period. Through
trackage rights agreements, both Amtrak and Union
Pacific
Railroad trains traversed
the
San
Bernardino subdivision east of Riverside
According
to the
ATSF
timetable, the maximum authorized speed for freight
trains on both the Cajon and the San Bernardino subdivisions was 55 mph On both
subdivisions
a train was restricted to 45 mph if it either weighed more than
7,000
trailing tons or had more than an average of 90 tons per operative brake.
Train 818 had a total of 8,616 trailing tons.
The Corona siding paralleled the main line for the siding's entire length,
8,507
feet. The
ATSF
timetable showed the Corona siding with
8,370
feet of
clearance^
available for safe train operations.
The Corona siding was intersected by four grade
crossings.
(See figure 1 ) The
first was Main Street, which was 565 feet from the east switch. The second was
Sheridan
Street, which was 1,786 feet from the east switch The third and fourth
were
Cota Street and Railroad Avenue, which were, respectively, 2,914 feet and
8,272
feet from the east switch
According
to the
ATSF
timetable, the authorized speed through the Corona
siding was 15 mph.
The General Code of Operating
Rules
specifies the actions that are to be taken
when one train is met or
passed
by another. Rule 89 states that "when a train is met
iSBecause
employees
living
in San
Bernardino
had so far to
travel
and because
traffic
congestion
in
the Los
Angeles
area
was
often
so bad, the
carrier
tried
to
give
employees
called
for
duty
at
Hobart
yard
2 1/2 to 3
hours
notice
of
their
reporting
times
The
engineer
of
train
818
received
his
calls
when
he was
home
2
hours
32
minutes,
on the average,
before
his
reporting
time
iSThe
clearance
is the
area
in
which
rolling
stock
and
locomotives
can
safely
clear
structures
and
equipment
on
adjacent
tracks
From Hobart Yard
From Barstow
Day
Date
Reporting Time
Time
on Duty Day
Date
Reporting Time Time on Duty
Hour Mm
Hour Min
Wed
5-Sep
5:00 AM 5
35
Wed
5-Sep
11:45 PM 8 40
Fn
7-Sep
4:45 AM
7
30 Sat
8-Sep
3:15 PM 2 30
Sun
9-Sep
4:15 AM S 30
Mon
10-Sep 12:15 PM 5 30 Tue
11-Sep
8:15 AM
6 30
Wed 12-Sep 11:00 AM
8
5 Thu 13-Sep
7:30 AM 6
30
Fn
14-Sep 5:15 PM
5
15 Sat 15-Sep
1.15 PM 6 30
Sun ! 16-Sep
Called 1449 Laid Off
On
Call
Mon i 17-Sep
8:30 PM 2
10
Dead Head Tue
18-Sep
8:00 AM
6 40
Thu
20-Sep 3:15 PM
8
50
Yard Job
Sat 22-Sep 4:15 AM
7
25
Sat
22-Sep
11:45 PM
5 45
Sun
23-Sep 5:15 PM
5
30 Mon 24-Sep
6:45 AM
7
0
Tue
25-Sep
7:05 AM 12 0
Thu
27-Sep
4:15 AM 6 0 Fn
28-Sep
2:15 AM
7
45
Sat 29-Sep
Called 1139 Laid Off Sick
Toe
2-Oct
10:00 AM
12 0
Thu
4-Oct
4:30 AM 9 30 Fn
5-Oct
3:45 AM
3 15
Dead Head
Fn
5-Oct
3:15 PM
8
0
Yard Job
Sat
6-Oct
Called 0415
Laid Off On Call
San
7-Oct
3:15 PM
8
0
Yard Job
Tue
9-Oct
2:00 AM
4
50
Tue
9-Oct
4:15 PM
2 20
Dead Head
Thu
11-Oct 12:30 AM
4
0
Dead Head Thu 11-Oct
7:15 PM 2 30
Dead Head
Fn
12-Oct 10:00 PM
2
20 Dead Head
Sat
13-Oct
8:45 AM 6
45
Sun
14-Oct
11:00 PM
2
30 Dead Head Mon
15-Oct 5:15 PM
6
30
Wed 17-Oct
4:15 AM 10 0 Thu
18-
Oct
12:15 AM 5 45
Fn
19-Oct 4:30 AM
10
0
Sat
20-Oct
3:20 AM
5
25
Sun 21-Oct
4:30 PM 5
45
Mon 22-Oct 8:45 AM
7 15
Tue 23-Oct
5:15 PM 5 0 Wed 24-Oct
12:15 AM 5
0
Thu 25-Oct Called 3:00 AM
Laid Off Personal
Sat 27-Oct 4:30 AM
7 0 Sun 28-Oct
12:15 AM
8 5
Mon
29-Oct 11:00 AM
6
15
Tue 30-Oct 1.15 AM
6
55
Wed
31-Oct 4:15 AM
8
30 Thu
1-Nov 12:01 AM
7
0
Fn
1
2-Nov
12:15 AM 7 25 Fn
2-Nov
3:45 PM 6 30
Sat i
3-Nov
10:30 PM
6 50 Sun
4-Nov
6:45 PM 12 0
Tue
6-Nov
4:30 AM S 10 Tue
6-Nov
10:15 PM
Collision At Corona at 4:10 AM
Source : ATSF
1
Chart By NTSB
Figure
5 -- Reporting times for the engineer of tram 818 at Hobart
Yard
and
Barstow
17
or passed
it
must stop and remain
not
less
than
400
feet from
the
signal
or
clearance
point
of
a facing point switch over which
a
train may
pass,
if
length permits."
In accordance with part
217.9 of
Title
49 of the
Code
of
Federal Regulations
(CFR),
the
ATSF
had
an
efficiency testing policy
for
testing operations employees
on
their knowledge
of
and compliance with its operating rules, timetable information,
and special instructions.
The
policy included guidelines
for 35
different
tests,
5 of
which
were about restrictive blocks
and
interlocking signals
One of the
tests
included operating rule
34,
"Observe
and
Call
Signals,"
which required
crewmembers
to
call signals
to
each other when they rode
in the
controlling
locomotive
According
to the
ATSF
regional manager, "most supervisors were required
to
make efficiency tests each month."
In
1990, supervisors in the subdivision performed
9,000
efficiency tests. About
10,000
trains traversed
the
subdivision during
that
period
of
time.
The
regional manager said
that
25
percent
of the
tests were
performed
at
night
All
crewmembers involved in the accident, with the exception
of
the brakeman
on train
818,
had been tested during the year before the collision. The engineer had
taken
76
tests He passed all
of
them, including two
that
were restrictive block signal
tests.
The conductor
of
train
818
had taken
24
tests with no failures.
The
engineer
of train
891 had
taken
36
tests, with
3
failures;
the
conductor
had
taken
70
tests,
with 1 failure; and
the
brakeman had taken
54
tests, with
3
failures. Cumulatively,
the five employees had taken
260
tests
ATSF
maintained hours-of-service records
for
all crewmembers involved
in the
accident. These records were in compliance with
49
CFR
Part
228.11.
The
ATSF
MOP testified
that
the carrier attempted
to
post
a
list
of
trains going
on duty on
a
4-hour
rotation via the
ATSF
system called
VIPS
The
ATSF
tried
to
have
the train line-up rotation information available
at 1, 5, and 9am and 1, 5, and
9
pm.
The
ATSF
regional manager testified
that
on
November
6, the
STO decided
on
the train line-up from Barstow
to
Hobart
at 4:17 p.m
and decided which crews were
to
be
deadheaded
at 515 p m.
The STO testified
that
on Tuesdays, and sometimes
on
Wednesdays,
crews were "invariably deadheaded due
to
traffic
cycles."
The crew calling office listed
on
VIPS
those crews being deadheaded
at
5.28 p m
The engineer
for
ATSF
818
had last checked the crew board when he went
off duty
at 12 40 p.m
By
contractual agreement,
the
ATSF
was required
to
issue "penalty
pay" to
employees
that
were held
at
their away-from-home terminal
16
hours beyond
the
time they went
off
duty.
The
carrier tried
to
avoid this occurrence whenever
possible.
Rule
G
of the
General Code stipulated
the
carriers' prohibition
of
alcohol
and
narcotics
on their property.
See
appendix
C
for
a complete definition
of
the rule.
18
Meteorological Information
According
to the
National Weather
Service,
the
ambient
air
temperatures
ranged from
56o
F
to 61o
F
at the
time
of the
collision Winds ranged from
12 to
19
mph; gusts ranged from
to 21 to 25 mph.
Temperature readings
and
wind
observations were taken
at
the three airports nearest the accident site
A
security guard who had been near the scene
of
the accident reported
on
local
wind conditions He described winds from
the
northeast
at 0 to 30
mph, "gusting
on
and
off
and blowing
a
lot
of
dust."
The conductor
of
train
891
indicated
it
was clear and breezy
in the
vicinity
of
the accident When specifically queried about the presence
of
blowing dust, he
said,
"I
don't believe so There might have been some,
but not
enough
to
obstruct
the
visibility."
He
reported
that
blowing dust was
not an
obstacle
to his
seeing
the
signal.
Also
interviewed were responding police officers,
who
reported
a
clear night
with
a
breeze Neither officer noted
that
his
vision
of the
collision scene
was
impaired by dust
Medical
and
Pathological Information
ATSF
818
Engineer.-According
to the
ATSF
medical files,
the
engineer received
his
last
physical
examination
on
March
23, 1990 He was
physically
fit for
duty
and was
issued
a
class
I
(unrestricted) medical certificate
As
part
of his
last
two
physical
examinations, his urine was screened
for
drugs, none were found
His
uncorrected
vision
was
20/15
(distant) and
20/10
(near),
he
had normal color vision
in
both
eyes
His
hearing was normal.
Conductor.-The conductor suffered from gastritis, which
he
had been treating
with
a
prescribed drug called Zantac
He
took
the
drug only
as
needed, which,
during
the
past
4
years,
was
infrequently.
He had
also suffered from headaches
during
the
past year, which his personal physician attributed
to
stress His wife said
that
he had not
been
ill
before
his
November
6
tour
to
Barstow,
nor had he
mentioned his health in the conversation he had with her while he was there
According
to the
ATSF
medical files,
the
conductor received
his
last physical
examination on April
19,1990
He was physically
fit for
duty and was issued
a
class
I
(unrestricted) medical certificate During
his
last
two
physical examinations,
his
urine was screened
for
drugs, none were found. His
vision,
corrected through
the
use
of
glasses,
was
20/20, he had
normal color vision
in
both
eyes
His hearing
was
last tested
on
October
5, 1989, he had
difficulty hearing high frequency sounds.
According
to
the
ATSF
medical director,
the
conductor's hearing was
not
outside
the
standards set by
the
American Academy
of
Audiolaryngology and
did not
preclude
him from performing his duties.
Brakeman.-The
ATSF
medical files indicate
that
she received
her
last physical
examination
on
October
17, 1990
She was physically
fit for
duty and was issued
a
class
I
(unrestricted) medical certificate During
her
last physical examination,
her
urine was screened
for
drugs, none were found
Her
uncorrected vision was
20/20
19
(near) and
20/22
(distant) Her color vision in both
eyes
was normal. She had a
hearing test on October
25,1990,
and
was
found to have normal hearing
ATSF891
Engineer.-The
ATSF
medical files indicate
that
the engineer received his last
physical
on March 23, 1990. He was found physically fit for duty and was issued a
class
I (unrestricted) medical certificate As part of his last physical examination he
underwent urine drug screening; the results were negative His uncorrected vision
was
20/50;
corrected by
glasses,
it was
20/20
in his right eye and
20/25
in his
left
eye.
He
had normal color vision in both
eyes
During his last hearing test, a slight
difficulty in hearing high frequency
sounds
was detected in his right ear.
Conductor --The conductor had reported
that
he was not sick on the day of the
accident.
He was taking two types of medicine The first was Ailopurinol, which was
prescribed for gout The carrier knew
that
he was using the drug The second was
Motrin, an over-the-counter drug, which he took for his arthritis. He had taken his
normal dose of Ailopurinol on the day of the accident and had taken a half dose (400
mg) of Motrin about 4 hours before the accident
According
to the
ATSF
medical records, his last medical examination was on
January
2, 1990. He was in good health and was issued a
class
I (unrestricted)
medical certificate His distance vision was
20/20
uncorrected in his
left
eye and
20/25
uncorrected in his right eye, his color vision was normal in both
eyes.
He had
difficulty hearing high frequency
sounds
with his
left
ear The examination included
a drug
screening,
and the results were negative.
Brakeman
--According to the
ATSF
medical file, he had his last physical on
November 7, 1989. He was physically fit for duty and was issued a
class
I
(unrestricted) medical certificate. His drug screen was negative. His uncorrected
vision
was
20/20,
and he had normal color vision in both
eyes.
His last hearing test
indicated
that
he had some difficulty hearing high frequency sounds with his
left
ear
Injuries
Fatal
--According to the Riverside County coroner's office, the three
crewmembers on train 818 died from smoke inhalation and thermal burns. The
evidence
of smoke inhalation was "soot in the airways " The autopsy surgeon
further reported
that
the brakeman's blood was "cherry red," indicating "carbon
monoxide intoxication." The autopsy report on the fourth fatality, the brakeman on
train 891, stated
that
he died of a severe head trauma
The engineer of train 818 suffered extensive thermal burns, diffuse charring of
his
body, and asphyxiation by smoke inhalation. His body was found approximately
20 feet northeast of the right rear corner of train 818's first locomotive.
The conductor of train 818 suffered extensive thermal burns, charring of his
entire body, and asphyxiation by smoke inhalation He had multiple injuries,
including lacerations of the liver, fractures of the right third through tenth ribs,
contusion
of the right lung, and subdural and subarachnoid hemorrhages His body
was
found about 15 feet west of train 818's lead locomotive on the south side of the
main track.
20
The brakeman
of
train
818
suffered extensive thermal burns, charring
of her
body,
and
asphyxiation
by
smoke inhalation.
Her
body was found about
20
feet
west
of
train 818's lead locomotive on the south side
of
the main track.
The brakeman
on
train
891
suffered
a
fracture
to the
base
of the
skull, brain
stem contusion, subdural and subarachnoid hemorrhages, extensive thermal burns,
and charring
of the
body His body was found
in the
control compartment
of the
train's third locomotive unit
Survivors.-The
engineer
of
train
891
sustained
a
concussion,
an
open fracture
of
the
right kneecap,
and
lacerations
of the
head
and
face
The
conductor
of
train 891 sustained bilateral comminuted fractures
of
the distal
tibia
and
the
fibula,
resulting
in
both ankles being broken
Both
surviving crewmembers were
hospitalized.
Toxicology
for
Drug Testing
In compliance with
49
CFR Part
219,
subpart C, blood and urine samples were
collected
from
the
survivors
of
train 891 and from the
ATSF
dispatcher
In
addition,
tests
were conducted on those who died.
The toxicology
on the
fatally injured crewmembers was reported
by
BioTox
Laboratory.
The carboxyhemoglobin (COHb) levels
in
three
of
the crewmembers
of
train
818
were
less
than
5
percent saturation;
in the
crewmember
of 891, it was
6 percent BioTox Laboratories sent the blood specimens
to
Poison
Laboratory, Inc
,
a clinical laboratory,
for
COHb analysis. According
to
telephone conversations with
the chief toxicologist
at
Poison
Laboratory, he was unaware
that
the specimens were
from fatally injured persons or
that
they were victims
of
a fire.
Blood
and
urine from
all
crewmembers and tissue specimens from
the
fatally
injured were sent
to
CompuChem Laboratories
to be
tested
for
drugs.
In
addition,
the Safety
Board
sent blood
and
urine from
all
crewmembers
to the
Center
for
Human Toxicology (CHT) Neither laboratory found
any
evidence
that
any of the
fatally injured crewmembers had taken illegal drugs.
CompuChem reported
that
the
urine taken from
the
conductor
of
train
891
contained
2,430
ng/ml
of
morphine
No
morphine was found
in his
blood.
The
conductor
had
received morphine
for
pain between
8 am. and 9.35 a m. on
November
7.
His blood
and
urine samples were collected
at
about
1 p m.,
almost
9 hours after
the
accident The CHT detected
a
morphine concentration
in
his urine
of
12,000
ng/ml Using
a
cut-off level
of 40
ng/ml,
it
did
not
detect morphine
in his
blood.
Blood
and
urine were collected from
the
engineer
of
train
891 at
about
3:30
p.m.,
11
hours after
the
accident CompuChem reported
that
his
urine
was
positive
for
methamphetamine
and
amphetamine
at
concentrations
of 457
ng/ml
and
88
ng/ml, respectively
At
the methamphetamine cut-off level
of 50
ng/ml,
his
blood
was
negative.
The CHT
reported
that
his
urine contained
587
ng/ml
of
methamphetamine,
117
ng/ml
of
amphetamine, and
8
ng/ml
of
the acid metabolite
of marijuana. Although CompuChem analyzed his blood, CHT did
not
have enough
of his blood
to
analyze.
21
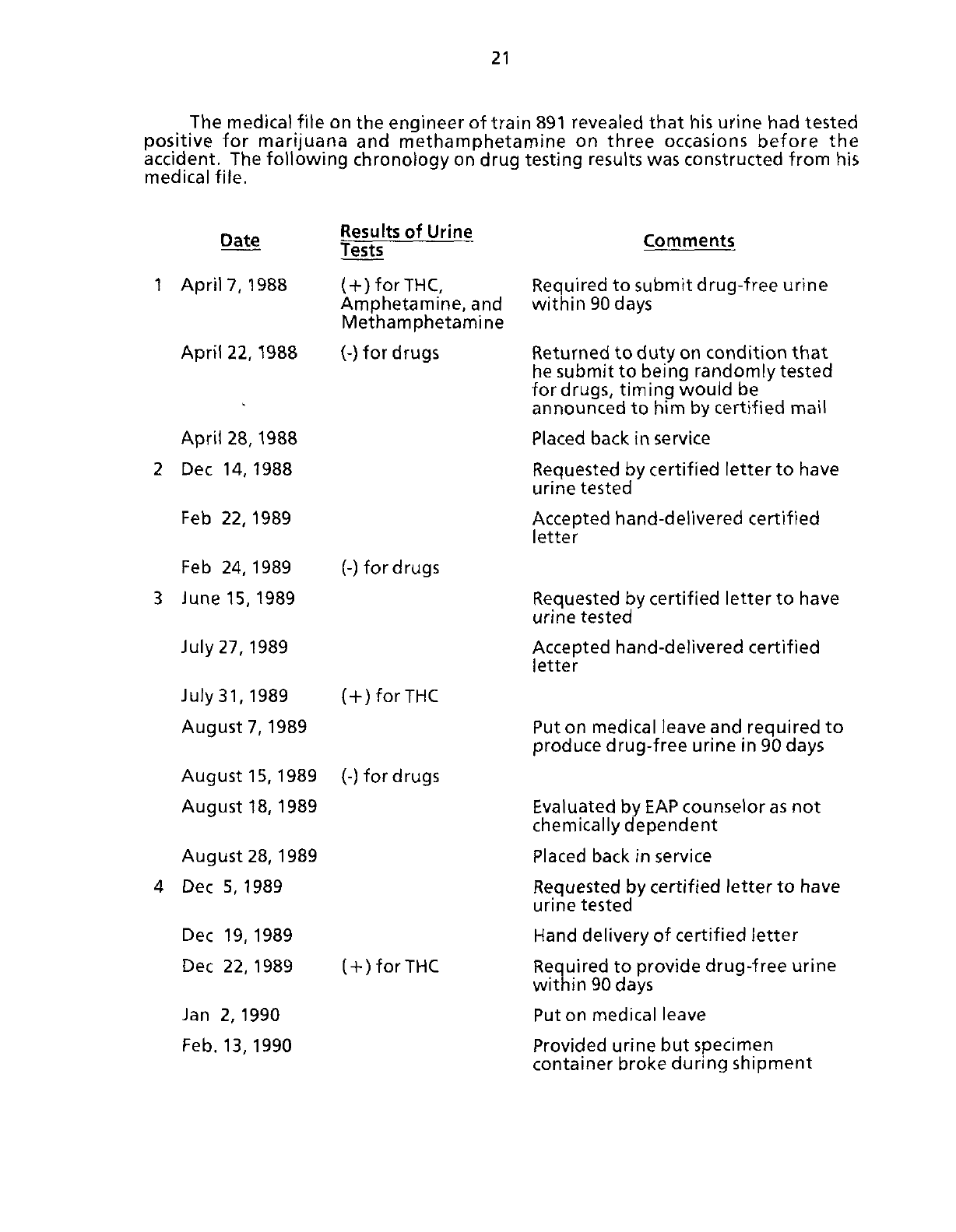
The medical file on the engineer
of
train 891 revealed
that
his urine had tested
positive
for
marijuana
and
methamphetamine
on
three occasions before
the
accident.
The following chronology on drug testing results was constructed from
his
medical file.
Date
Results
of
Urine
Tests
Comments
1
April
7, 1988
(-f-)forTHC,
Amphetamine, and
Methamphetamine
April
22,1988 (-) for
drugs
April
28,1988
2
Dec 14, 1988
Feb
22, 1989
Feb
24, 1989 (-)
for drugs
3 June
15,1989
July
27, 1989
July
31,
1989
(
+
)forTHC
August
7, 1989
August
15, 1989 (-) for
drugs
August
18, 1989
August
28, 1989
4
Dec 5, 1989
Dec
19, 1989
Dec
22, 1989
(
+
)
for THC
Jan
2,1990
Feb.
13, 1990
Required
to
submit drug-free urine
within
90
days
Returned
to
duty on condition
that
he
submit
to
being randomly tested
fordrugs, timing would
be
announced
to
him by certified mail
Placed
back in service
Requested
by certified letter
to
have
urine tested
Accepted
hand-delivered certified
letter
Requested
by certified letter
to
have
urine tested
Accepted
hand-delivered certified
letter
Put
on medical leave and required
to
produce drug-free urine in
90
days
Evaluated
by
EAP
counselor
as
not
chemically
dependent
Placed
back in service
Requested
by certified letter
to
have
urine tested
Hand delivery
of
certified letter
Required
to
provide drug-free urine
within
90
days
Put
on medical leave
Provided
urine but specimen
container broke during shipment
22
Date
Results
of
Urine
Tests
Comments
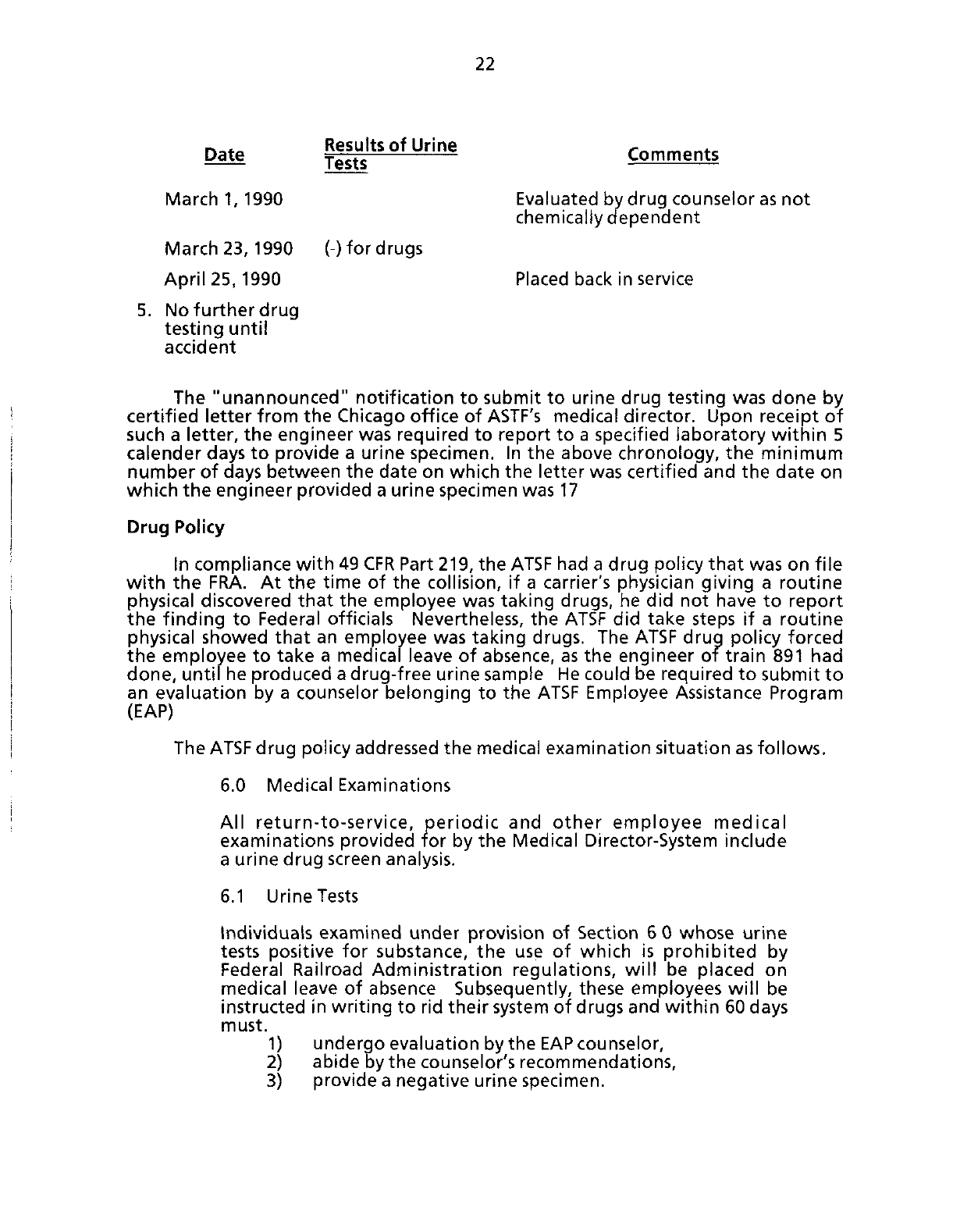
March
1,1990
Evaluated
by drug counselor as
not
chemically dependent
March
23,1990 (-) for
drugs
April
25, 1990
Placed
back in service
5. No further drug
testing until
accident
The "unannounced" notification
to
submit
to
urine drug testing was done
by
certified letter from
the
Chicago office
of
ASTF's
medical director. Upon receipt
of
such
a
letter,
the
engineer was required
to
report
to a
specified laboratory within
5
calender days
to
provide
a
urine specimen.
In the
above chronology,
the
minimum
number
of
days between
the
date on which
the
letter was certified and
the
date
on
which
the engineer provided
a
urine specimen was
17
Drug
Policy
In compliance with
49
CFR Part 219, the
ATSF
had
a
drug policy
that
was on file
with
the
FRA.
At the
time
of the
collision,
if a
carrier's physician giving
a
routine
physical
discovered
that
the
employee was taking drugs,
he did not
have
to
report
the finding
to
Federal officials Nevertheless,
the
ATSF
did
take steps
if a
routine
physical
showed
that
an
employee was taking drugs. The
ATSF
drug policy forced
the employee
to
take
a
medical leave
of
absence, as
the
engineer
of
train
891 had
done,
until he produced a drug-free urine sample He could
be
required
to
submit
to
an evaluation
by a
counselor belonging
to the
ATSF
Employee Assistance Program
(EAP)
The
ATSF
drug policy addressed the medical examination situation as follows.
6.0
Medical Examinations
All
return-to-service, periodic
and
other employee medical
examinations provided
for
by the Medical Director-System include
a urine drug screen analysis.
6.1 Urine Tests
tndividuais examined under provision
of
Section
6 0
whose urine
tests positive
for
substance,
the use of
which
is
prohibited
by
Federal Railroad Administration regulations, will
be
placed
on
medical leave
of
absence Subsequently, these employees will
be
instructed
in
writing
to
rid their system
of
drugs and within
60
days
must.
1) undergo evaluation bythe
EAP
counselor,
2) abide by the counselor's recommendations,
3) provide
a
negative urine specimen.
23
An
employee in a treatment program extending beyond the 60 day
period must provide a negative urine specimen within five (5) days
of discharge from the program Failure to abide by these
conditions will subject the employee to dismissal for disobeying
instructions.
A
decision by the Medical Director-System to withhold an
employee from service under Section 6 of this policy is not and shall
not be considered discipline
6.2 Follow-Up-Testing
An
employee who provides a negative urine specimen and has
been permitted to return to service is subject, for a period of two
(2)
years,
to urine testing as determined by the Medical
Director-System If such further testing is positive, the employee
will be placed on medical leave of absence.
Such
an employee will
be subject to the same conditions set forth in Section 6.1.
On March 1, 1991, the
ATSF
issued a new drug policy, any employee could be
fired the second time that tests, including those given during a routine physical,
showed
that he had been taking drugs
Fire
A
postcollision fire enveloped both equipment and personnel. The fire was
fed by diesel fuel that spilled from two ruptured locomotive fuel tanks Some of
the fuel had been sprayed into the air, making it highly combustible.
Postaccident
Damage Examination
The on-site investigation did not reveal any anomalies in the braking system
of either train
The
left
front end sill area of the lead locomotive on train 818 collided with
the
left
front end sill area of the lead locomotive on train 891 The lead locomotive
of train 818 incurred damage due to the collision and subsequent fire The
superstructure of its control compartment had sustained thermal damage and
showed
crush damage from the front end sill rearward for approximately 15 feet
The locomotive remained on its trucks in the turnout on the west end of the siding,
and its fuel tank was intact. (See figure 6) The first, third, fourth, and
fifth
locomotives of train 818 had derailed
The electrical switches in the control cab were burned, but investigators were
able to document the following, rear headlight switch off, gauge lights on, front
headlight on in dim position, generator field switch not discernible, engine run
switch
not discernible, side wall heater switch on high, and throttle next to the
"idle stop" position The brake systems of all units were also inspected and found
to be functioning
as
designed.
In an attempt to determine the approximate point of the emergency air brake
application, investigators measured from the initial discharge of air brake sand to
the collision point The sand
trait
began approximately 60 feet before the collision
point The sanding system sequence is designed to automatically begin to
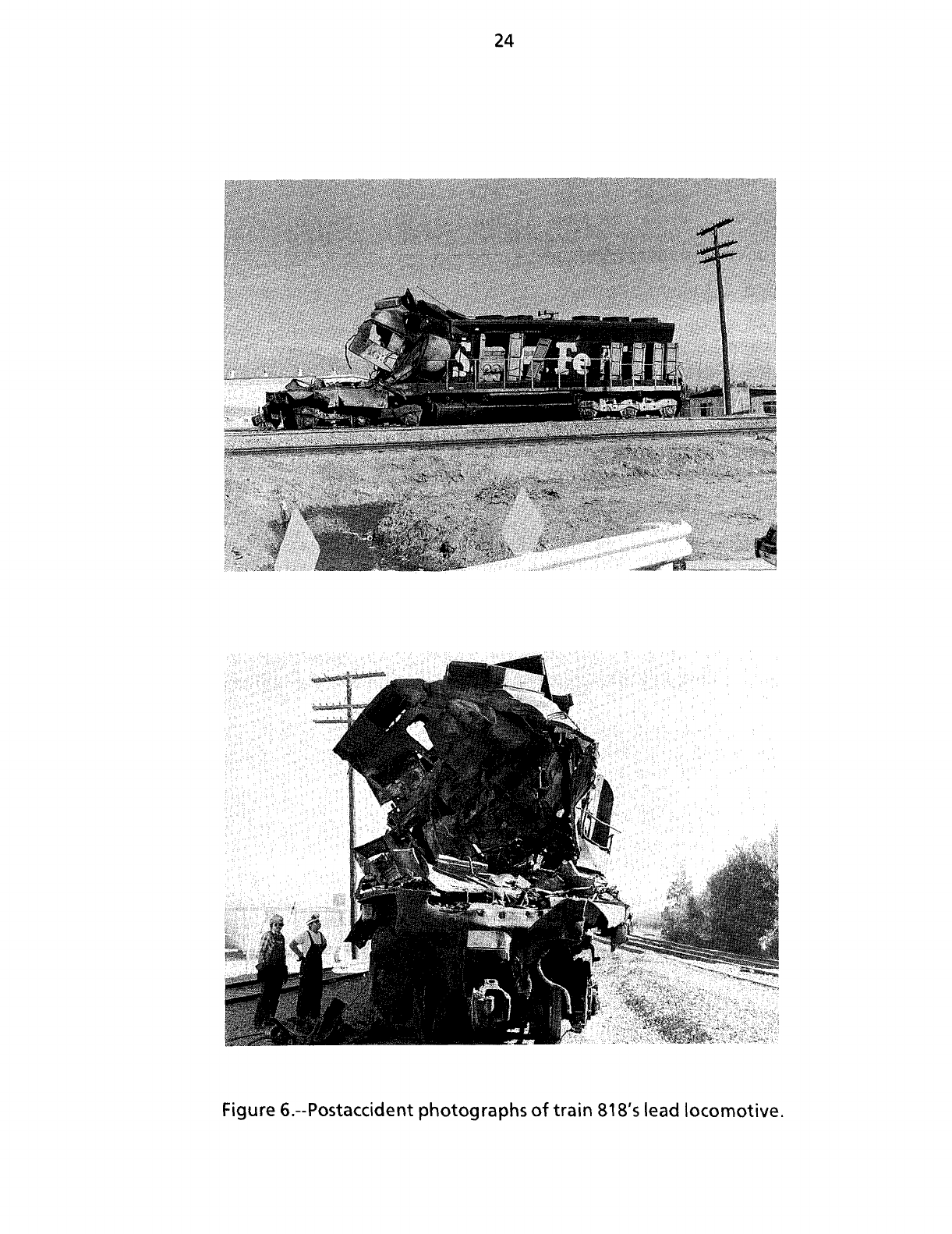
24
ure 6.--Postaccident photographs of
train
818's lead locomotive.
25
discharge
its contents when an emergency brake application is initiated. There is
an
inherent time lapse within the system.
The 12th, 13th, and 14th rail
cars
were involved in a derailment
that
was
subsequent to the collision.
All
three locomotives on train 891 derailed, as did the first, second, third, and
fourth rail
cars
The 31st rail car subsequently derailed due to the collision
The lead locomotive of train 891 showed minor damage on its
left
front; its
pilot, fuel tank, and both trucks separated from its underside It also had collision
marks 57 1/2 inches inboard on the
left
side of the
119-inch
wide locomotive
pilot/snowplow. Paint marks on the
left
side of its nose were the same color as the
paint on the lead locomotive of train 818. Investigators noted
that
the unit had
been hit on the front-end sill area and
that
the first impact was on the underframe
of the anticlimber
system.
The second locomotive of train 891 showed major thermal damage. Its "B"
end (rear end) was bent downward and pushed forward. The
left
side showed
moderate crush damage, and the
left
side of the control compartment's roof had
collapsed
downward approximately 10 inches. The interior of the control
compartment was completely destroyed by fire.
Both
trucks had separated from
the underside, the fuel tank, although ruptured, remained attached to the
underframe.
The third locomotive of train 891 also showed major thermal damage. The
left
side of the control compartment showed moderate crush damage The interior
of the control compartment was completely destroyed by fire and the fuel tank
remained attached to the underframe and was ruptured.
Both
trucks had
separated from the locomotive.
The collision damaged the main track and the Corona siding. Approximately
135 feet of the main track were damaged, as were 291 feet of the track and a
number 10 turnout in the siding. The switch points and connecting rods of the west
end siding turnout were also damaged.
The positions of all relays of the signal system were documented. When the
positions
were checked against the signal circuit plans, it was noted
that
signal 2R,
the signal governing train 891's progress, was displaying a green aspect and
that
signal
2LB,
the signal governing train 818's movement, was displaying a red aspect.
Signal
2LB had been struck before the accident, causing its mast to lean
toward the track at about 5 degrees from vertical. No equipment or debris
resulting from the collision
was
found in the vicinity of the signal
The power-operated switch machine was undamaged and mechanically
locked
in the normal position, lined for main track traffic; the normal indication
contacts
were closed
The wig-wag grade crossing signal was about 80 feet east of the collision
point and was still activated when investigators arrived on the scene 12 hours after
the collision.
26
Survival
Aspects
Emergency
Response --About 4
1
15 a.m the Corona police and fire dispatcher
received
a telephone call from a private citizen about a rail car fire in the area of
Railroad
Avenue and Smith Street. The accident was simultaneously reported to
the California Highway Patrol by the Corona police Between 4:15 a.m and
4.24 a.m., one battalion chief, four fire engines, one rescue unit, and one
ambulance were dispatched to the scene The fire, except for the burning cargo,
was
under control within an hour.
The Corona police department also responded. According to the police
report, 17 units with 18 supervisors and officers were initially dispatched to the
accident site. Their duties included documenting the
scene,
interviewing witnesses
and train crewmembers, and controlling the traffic and the accident site perimeter
By
4:29 a.m., the police and fire departments had established a joint
command post at the 1300 block of Railroad Avenue. The post was staffed until the
afternoon of November 9 The fire chief was the incident commander
Crashworthiness
-None of the locomotives involved in the accident sustained
a direct frontal impact. No survivable space was left in the control compartment of
the lead locomotive unit on train 818 as a result of the accident The bulk of the
damage to the conventional cab of this unit was caused when train 89Vs third
locomotive came to rest on top of the control cab of the lead unit on train 818
The North American cab locomotive on train 891 maintained its structural
integrity throughout the collision No intrusions were noted to the cab areas of the
GP-60M locomotives other than a minor dent in the roof area on the engineer's side
of the lead unit, which was the result of the locomotive's falling on its
side.
There
was
survivable space for all occupants in the control compartments of the GP-60M
locomotives
Pipeline
Information
Natural Gas Pipeline --The
ATSF
main track at Corona was flanked on its north
side
by a 30-inch diameter natural gas pipeline that belonged to the Southern
California Gas Company. At the time of the accident the line pressure was
554 pounds per square inch in gauge
(psig)2o
The line was still under pressure
when the investigating team arrived on the scene and was shut in2i at
1
10 a.m. on
November 8.
20
Gauge
pressure
is the
difference
between
the
total
absolute
pressure
and the
atmospheric
pressure
(14 7
pounds
per square
inch
absolute)
21A
segment
of
pipeline
is
considered
to be
shut
in when
pressurized
liquid
or gas is
contained
within
the
segment
by
closed
valves
27
Petroleum Pipeline.-A 16-inch diameter crude oil transmission pipeline
operated by the Four Corners
Pipe
Line Company flanked the south side of the main
track.
ltwasshutdown22at7a.m
on the day of the accident
Tests
and Research
On November 21, two members of the mechanical group and designated
personnel from the FRA and the
ATSF
met at the
ATSF
Topeka,
Kansas,
air brake
shop
to examine and test the air brake equipment from the lead locomotive of
train 818 The automatic brake valve was removed and examined. Investigators
found that the automatic brake handle shaft inside the engineer's stand was in the
emergency position.
ATSF
records indicated that predeparture air brake tests and
safety appliance inspections had been conducted at Barstow and Hobart yards and
that both trains were in compliance with applicable railroad and FRA requirements
The horns from the lead locomotives of both trains were also tested by
investigators and were found to be operational.
The Safety
Board
and the
ATSF,
using the Association of American Railroads
Technical Center
(AARTC)
in Chicago, ran computer simulation tests to determine
how the time required for each train to come to a complete stop varied according
to its speed. Ten tests were made on a simulated train 818; during the tests, the
speed
of the train ranged from 4 to 8 mph Twelve tests were made on a simulated
train 891 with speeds ranging from 25 to 35 mph. All 22 simulations took into
consideration the tonnage and length of the trains, as well as the degree of grade
of the respective tracks
The tests showed that when the speed of train 818 was between 4 and 6 mph,
it required a minimum of 32 feet and a maximum of 116 feet to come to a complete
stop after the emergency brake application.
According
to the testimony of the conductor of 891, the train was about 5 car
lengths (a car length
is
about 75 feet), or about 375 feet, west of the 2R signal when
the engineer noted that the signal had changed to a red aspect. The train traveled
44 feet before the engineer was able to do anything, assuming that it took him 1
second
to react and initiate emergency braking and that the train's speed was
about 30 mph
The reaction of the air in an emergency braking application within the train's
braking system was at a rate of 930 feet per
second.
Since
train 891 was
4,229
feet
long,
it would have taken about 4 1/2 seconds for the air to travel from the lead
locomotive to the last rail car Tests showed that at 30 mph, train 891 would have
required between approximately 870 and 990 feet to come to a complete stop after
the emergency brake application.
Sight
Distance -On November 9 at 5.10 a m , the Safety
Board
conducted
sight/distance tests at the accident location It was dark, clear, and calm; and the
temperature was about 50o F. The same kind of locomotives were used as those
22
A
segment
of
pipeline
is
considered
to be
shut
down
when
pumps
or
compressors
have
been
stopped
and
pressure
in the
pipe
remains
constant
28
that
the train had on the night of the accident. The tests showed
that
when train
818 was in the siding, the stop signal could be
seen
at a distance of 1,391 feet.
The
maximum
distance from which crewmembers of train 891 could have first
seen
the headlight of train 818 was over 1,300 feet west of the collision point
Signal
System --Although signal 2LB was leaning south, its focal point was
clearly
visible even in darkness at a distance of over 1,300 feet An electrical
breakdown test of all control circuitry at west Corona was conducted on
November 7, and no defects were found.
The control circuitry for operating the two wig-wag crossing warning signals
at Railroad Avenue was also tested and found to be functional
On
November 9, a breakdown test of the signal system was conducted
that
included clearing signals, simulating the reversing of the switch, and simulating
train moves. The signal system functioned
as
designed and within the guidelines of
the FRA rules and regulations governing railroad signal and train control systems
No defects were found
Event
Recorders.-On the day of the accident,
ATSF
personnel removed the
event recorder data pack from train 818 and sent it to their Barstow engine facility.
The
next
day, at the request of the Safety
Board,
the carrier gave the data pack to
the investigator-in-charge, who in turn sent it to the Safety
Board's
laboratory in
Washington,
D.C.
The event recorder was on the
fifth
locomotive, it used a magnetic tape and
recorded eight events. The events recorded were time, speed, locomotive
amperage, direction of travel, automatic brake pressure, locomotive brake
application,
throttle, and dynamic brake application.
The Safety
Board's
laboratory noted
that
the dynamic braking was off, the
throttle
had dropped to zero, and an emergency application was made to the
train's braking system just before the collision. The laboratory also noted
that
the
train's speed was about 14 to 15 mph from the time train 818 entered the siding
until about 2 1/2 minutes before the collision, approximately 10 to 15 seconds
before the
collision,
its speed decreased to about
5
to 6 mph .
The event recorder data did not indicate whether the emergency application
was
initiated by the automatic brake valve or by the emergency brake
valve.
After
the emergency application was made, the train moved about 80 feet west and
either had stopped or was about to stop at the time of collision. According to the
laboratory, there was a variable time lapse of 5 3/4 to 11 112 seconds between the
time
that
certain events took place and the time they were recorded The time
lapse
was in accordance with the manufacturer's specifications The events
affected by the time delay were
throttle
movement, automatic brakes, locomotive
brakes,
and direction of travel.
Between
the San Bernardino yard and the east switch of the Corona siding
(approximately 22 miles), the speed of the train exceeded 45 mph (maximum
authorized train speed) 13 times.
29
The event recorders on train 891 were destroyed in the fire They were
housed
in a metal container designed by the manufacturer and located in the
vestibule
of the control compartment.
Information about how the train had been handled was derived from the
conductor's
testimony Consequently, vital information about
such
topics as
braking,
throttle
manipulation, and the chronological relationship of events before
the accident was not available.
Natural Gas Pipeline --On November 7, the Southern California Gas Company
(SCGC)transmission
department surveyed for extensive leakage and did a pothole
inspection in the vicinity of the collision
On
November 9, while the line was out of
service,
(SCGC)
made a hydrostatic
test on
that
portion of the line in the derailment area
Petroleum Pipeline --The Four Corners
Pipe
Line
Company
(FCPLC)
shut down
its
line and replaced 115 feet of the line
that
was in the vicinity of where the lead
locomotive of train 891 landed
Both
pipelines were undamaged by the collision
Other Information
Pipeline
Notification -The
ATSF
did not directly notify either pipeline
operator of the accident. The natural gas line operator was notified by the Corona
police
department, and the petroleum operator was notified by the California State
Fire
Marshal's office. According to the
ATSF,
it did not notify the operators because
it knew they had been notified by the fire and police departments.
An
emergency accident response form was used by the MOP or the STO on
duty when an incident occurred as a checklist and an informational tool (See
appendix F)
On
the form, the western region was organized according to mile post
reference points When an accident occurred, the MOP or STO referred to the form
for the names of the emergency and carrier personnel who were responsible for the
area affected by the incident The form did not include the telephone numbers of
either the
SCGC
or the
FCPLC
Locomotive
Fuel
Tank.-The integrity of locomotive fuel tanks has been
compromised in several recent accidents
23
During the postaccident investigation of this collision, the Safety
Board
noted
that
the fuel tanks on both the first and third locomotives of train 891 were
ruptured and
that
their contents had been released. During the collision, one tank
had been punctured by a set of wheel trucks, and the other had been ruptured
either by debris or by the impact of landing on top of the lead locomotive of
train 818.
23The
accidents
investigated
by the
Safety
Board
in
which
locomotive
fuel
tanks
were
compromised
were
Sugar
Valley,
Georgia
(DCA90MR008),
Baker,
Oregon
(LAX90FR015),
Roebuck,
South
Carolina
(NYC91FR004),
Lompoc,
California
(LAX91FR009), and
Baltimore,
Maryland
(NYC91FR019)
30
The exterior shells of the fuel tanks were made of
3/16-inch
mild steel with
1/2-inch
end plates The tanks were installed between the wheel trucks underneath
the locomotives' underframes.
The Safety
Board
questioned the EMD representative about past studies
pertaining to the crashworthiness of fuel tanks. The
EMD's
senior project engineer
testified
that
his company ". . . had been doing some investigation on the
possibilities in trying to develop a tank
that
would
limit
the amount of spillage.
But,
it's an extremely difficult and complicated arrangement, and that's about as
far
as
we've gone at this point"
The Safety
Board
asked both the FRA and the Association of American
Railroads
(AAR) about fuel tank crashworthiness and was unable to find any data
pertaining to this subject
Positive
Train Separation System.--Railroad collision avoidance has been one
of the most frequently discussed
issues
at the Safety
Board.
Since
the
1970s,
the
railroad industry has been studying how the new technology in computers and
communications could be used in train control systems to prevent one train from
colliding with another. Canadian and U.S. railroads have jointly examined this
idea; and the AAR currently manages the project. The project is called the
advanced
train control system
(ATCS)
Several
U.S. railroads have actively pursued the
matter
and have
experimented with systems on their respective properties These systems use
on-board computers to monitor the actions of a train and automatically stop a train
if the engineer fails to comply with a signal. Neither train 818 nor train 891 had a
computerized collision avoidance system.
ANALYSIS
General
Neither the track nor the wayside signal system was a causal factor in the
accident. Neither the locomotives nor the rolling stock of the trains had mechanical
defects
that
would have contributed to the accident.
The train crewmembers were qualified for their positions The physical and
medical conditions of the conductor and the brakeman of train 891 were not
factors in the accident
Accident
Train 891 was traveling east on the main track approaching Corona and
operating in accordance with the carrier's timetable.
At the same time, train 818 was traveling west. It entered the Corona siding,
which
was adjacent to the main track, at a speed of 15 mph According to the event
recorder printout, from about 7 1/2 minutes before the collision until about
2
1/2 minutes before the collision, the train averaged about 14 to 15 mph; and then
its speed gradually decreased to about 6 mph about 10 to 15 seconds prior to the
collision.
An emergency brake application was made after train 818 passed the 2LB
dwarf signal about 10 seconds before the collision. Train 818 entered the main
31
track and blocked the progress of train 891; at 4:11 a.m., the lead locomotives of
both trains collided head on
Based
on the information from tests done at the
AARTC,
train 818 could have
traveled a
maximum
of about 116 feet between the time the brake was applied
and the time of the collision The Safety
Board
concludes
that
if the application
occurred
when the train was abreast the stop signal, about 120 feet from the main
track, the train probably would not have obstructed the clearance of the eastbound
train on the main track.
Train 891 was about 375 feet from signal 2R when it suddenly turned red.
Tests
showed
that
it would have taken about 830 to 990 feet to come to a complete
stop.
Therefore, the Safety
Board
concludes
that
when the lead locomotive unit of
train 818 entered the clearance area of the main track, there was not enough
distance
between it and train 891 to allow train 891 to come to a complete stop.
Based
on event recorder data, the position of the automatic brake
valves,
and
the approximately 60 feet of air brake sand found alongside the lead locomotive,
the Safety
Board
concludes
that
train 818 had either stopped or nearly stopped at
the time of the collision.
Because
the engineer, the conductor, and the brakeman of train 818 did not
take timely action to stop the train for the stop signal, the Safety
Board
examined
several
factors
that
may have affected their performance. These factors included
the work/rest
cycles
of the engineer and the conductor, the decisions of the
engineer and the brakeman about when to sleep, and the decision of the engineer
about whether to accept the work assignment.
Work/Rest
Cycles
Engineer
of train 818 --An extensive examination of the engineer's work/ rest
cycle
during the 90 days preceding the accident revealed a wide variation in his
reporting times. The purpose of the examination was to determine to what
extent
the fluctuations in his schedule may have affected the events leading to the
accident.
Near the beginning of the
90-day
period, the engineer took a
3-week
vacation,
thereby changing his employment-induced work/rest
cycle.
Consequently, the Safety
Board
focused on the 64 days from his first day back at
work, September 5, through the day of the accident, November 7
The engineer returned from vacation to his previous freight pool assignment,
which
required him to operate trains between Hobart yard and Barstow. He
remained in the freight pool service for 12 days and then transferred to the
extra
board.
He remained on the
extra
board for 3 weeks, after which he transferred
back
to freight pool service
During the
64-day
period, he worked 47
days,
averaging 7 hours 26 minutes
on
duty in a calendar day However, during the 47 days
that
he worked, he was
called
to duty 56 times, meaning
that
on 7
occasions
he worked 2 tours of duty on
the same calendar day
His
work schedule was irregular, his duty hours ranged from as few as 2 hours
10 minutes (when he was deadheaded) to as many as 12 hours (when he was
32
operating a train) The amount of rest he had between tours of duty was
correspondingly irregular, it ranged from
as
few as 2 hours to as many
as
96 hours.
His
work/rest periods were unpredictable In 54 tours of duty, he had 35
different reporting times. During 14 tours, he worked between 8 am. and 4 p m.;
during 15 tours, he worked between 4 p.m. and 12 a.m., and during 25 tours, he
worked between 12 am and 8 a.m.
On
25
occasions
he reported to work 8 hours or more later than he had on the
previous
day, meaning that he changed shifts 46 percent of the time. Figure 4
summarizes this information.
Sleep
research suggests that the human body maintains an approximate
day-night
cycle
known as circadian rhythm
24
Researchers have noted the effect of
violating the circadian rhythm.
the quality and quantity of sleep is degraded and
performance is impaired as a result of working at night. These
changes
are primarily caused by the disharmony between the
night worker's schedule and the underlying circadian rhythms
of the body The two are completely out of phase The body is
programmed to be awake and active by day and asleep and
inactive
by night, and it is extremely difficult to adjust this
program in order to accommodate artificial phase shifts in the
sleep-wake
cycle.25
Thus,
the biological clock regulating bodily functions and actual time are out
of synchronization for workers with schedules like the engineer's
Also,
their
biological clocks do not adjust quickly or easily to changes in the timing of their
sleep
that are imposed on them by irregular shift work The engineer hinted at this
problem in his
12-minute
conversation with the STO when the STO asked him if he
had his rest He replied, "Well
yeah,
we've had what they called rest off, but can
you
force yourself to lay down and go to sleep when you are not tired?"
Indeed,
research^ has shown that shift workers never fully adapt to irregular
night shift routines Workers have difficulty working at night, which the body
normally
reserves
for
sleep,
and sleeping during the day, when the body is normally
awake.
When duty times are unpredictable as well as irregular, the conflict can be
intensified.
As
a result of this these conflicts, shift workers begin to suffer physiological
changes
and to experience job performance decrements Significant decrements
have
been observed in visual acuity, cognitive functions, memory, reaction time,
and,
particularly, vigilance levels across extended time periods As alertness
24Grcadian
rhythm
is a
term
used
to
define
cyclical
biological
processes
which
occur
at
approximately
24-hour
intervals
in
approximate
synchrony
with the
earth's
day/night
cycle
Sleep/wake
patterns,
body
temperature,
hormone
levels,
and
metabolism
are
some
of the
processes
that
have
recurring
and
predictable
variations
throughout
a
24-hour
period
25Tilley,
A J , et al "The
sleep
and
performance
of
shift
workers
"
Human
Factors,
1982, 24
629-641
26Mitler, M M , et al
Catastrophes,
Sleep and
Public
Policy
Consensus
Report
Sleep, 1988,
M
No. 1
100-109
33
decreases,
reaction time increases, and the quality of judgment and decisions
decreases
Dr Donald Tepas27 noted that studies of industrial workers have shown that
people who work irregular shifts sleep
less
and also report more frequent sleep
problems than do people who work regular daylight shifts.
Conversations
with shift workers and other anecdotal evidence have shown
that it can be difficult for a person to go to sleep when his schedule calls for it but
his
body does not. If he does manage to fall asleep, he may not be able to stay
asleep
as long as he should. Consequently, shift workers fail to obtain a sufficient
amount of quality sleep and develop a sleep deficit that cannot be made up This
accumulation of sleep deprivation
causes
chronic28 fatigue, which they are unlikely
to recognize unless they have had specialized training
Chronic
sleep deprivation manifests itself in microsleep and napping. A
microsleep is defined as a brief involuntary period of sleep that lasts from a few
seconds
to minutes and ends spontaneously. A microsleep can be disrupted by
external stimuli, but only if they are massively sensory in nature, very unusual, or
particularly meaningful. Microsleeps increase in frequency and duration as the
loss
of sleep increases The worker may have no warning of either the beginning or end
of a microsleep; when he
has
finished his microsleep, he may not even know that it
has
occurred.
The onset of sleepiness that arises from chronic sleep deprivation is to some
degree predictable. Research29 indicates the existence of a circadian nadir, which
occurs
between approximately 1am and 7 a m., and a secondary trough, which
occurs
between 1 p.m, and 5pm These are periods of diminished capacity for all
workers,
even those who are well rested. However, a worker's ability to resist their
effects is greatly reduced when he has not slept, and it is during these periods that
he
is likely to microsleep.
If the work environment lacks stimulation, the worker is more likely to fall
asleep
For example, according to a Dinges study:
Driving,
no matter what the vehicle, seems especially prone to
drowsiness,
errors, missed signals, and accidents at the
predicted times A
study^o
of
2,238
failures to respond to
warning switches (which then induced automatic braking) by
15,000
German train drivers revealed a temporal function with
two peaks, 3am and 2pm
27Dr Tepas
testified
before
the Safety Board
during
the
public
hearing
regarding
the
collision
of two
Consolidated
Railroad
Corporation
freight
trains
Please
refer
to "Head-End
Collision
of
Consolidated
Rail
Corporation
Freight
Trains
UBT-506 and TV-61
near
Thompsontown,
Pennsylvania,
January 14,
1988 " NTSB/RAR-89/02,PB89-916302
28Chronic
fatigue
is
attributed
to
accumulated
sleep
deprivation
due to
circadian
disharmony
(violation
of
sleep/wake
cycle) or
circadian
desynchronosis
(rapid
crossing
of
time
zones)
29Dinges,
DF, "The
Nature
of Sleepiness Causes,
contexts,
and
Consequences
"
Chapter
9 in
Stunkard,
A J , Baum, A eds Perspectives in
Behavioral
Medicine.
1988, 162
3
0Hildebrandt,
G , et al
"Twelve
and
24-hour
rhythms
in
error
frequency
of
locomotive
drivers
and
the
influence
of
tiredness
"
International
Journal of
Chronobioloqy,
1974, 2,
175-180
34
15,000
German train drivers revealed a temporal function with
two peaks, 3 a.m. and 2 p.m
The engineer of train 818 experienced chronic (long-term) sleep deprivation
because
of the irregularity and unpredictability of his work/rest
cycle.
In addition,
the chance
that
he would fall asleep was greatly increased by the fact
that
he had
so
little
sleep before he started the
trip
After awakening on November 5, he stayed up about 4 hours and had dinner
with his family before going to bed for the night. He slept for 5 1/2 hours before
receiving
a call to work again at
1
"30 a m on November 6 He did not go back to
sleep,
but dressed and drove to work Thus, he began the tour of duty with
insufficient sleep and at a time of day when, according to his circadian rhythm, he
should
have been asleep. The
trip
to Barstow was, however, successfully
completed.
In the 26 hours 41 minutes between the time he was called to work, 1.30 a m.,
November 6, and the time of the accident on November 7, he had had very
little
sleep
The
maximum
amount of sleep he could have had from the time he finished
speaking to the STO until the time he
left
the Barstow motel to go to work was
1
hour 6 minutes (8.54 p.m to 10 pm.).
After being awake for more than 26 hours, the debilitating effects of sleep
loss
were high and they were greatly enhanced by his working during the low point
of his circadian rhythm. These effects may have caused the fluctuation in the speed
of the train between San Bernardino and the siding at Corona During this period
of time, train 818 exceeded the
maximum
speed 13 times
He
had his last radio communication with the San Bernardino dispatcher
about 3:52 a m , when he acknowledged instructions to take the siding at Corona
and allow the eastbound train to
pass.
According to the event recorder printout, a
reduction was made to the train's braking system about 4-03 a.m. in order to slow
the train to 15 mph The last action performed on the engineer's stand was about
4-11 a.m , when the
throttle
position changed from dynamic braking to
zero
throttle
Other than having to sound his horn at each grade crossing, there were no
other performance demands on him until the train reached the signal at the west
end of the siding. The engineer sounded the horn at Cota Street, which was
5,358feet
from Railroad Avenue, where an emergency brake application was
made.
Since
he sounded the horn, he must have been awake at Cota Street
However,
the emergency brake application occurred when the train was beyond
the stop signal and in the vicinity of the wig-wag grade crossing protection device,
as
indicated by the trail of air brake sand found on the track structure west of the
stop signal. The Safety
Board
concludes
that
train 818 traveled over 25 feet from
the point when the emergency brake application was initiated to when the sand
began to spread onto the rail, based on the speed of the train coupled with the
sanding system sequence.
It is likely
that
the rhythmic sound and motion of the locomotive's engines,
the lack of physical activity, and a cab heater turned on full further produced an
environment conducive to sleep The fact
that
the engineer had opened the cab
window and turned on the interior dome light on the engineer's side suggests
that
he
tried to keep himself awake.
35
Nevertheless,
the
Safety
Board
believes that his efforts to stay
awake
were
unsuccessful.
As
stated in
onestudy;3i
when
sleep is lost or disrupted, by whatever
means,
the
inevitable
consequence
is
sleepiness
during the wake period. If
sleepiness
becomes
excessive,
the person
ceases
to function
effectively
because
ultimately the brain imposes
sleep,
typically
in the form of overwhelming drowsiness or microsleeps,
despite
the individual's best efforts to stay
awake
The
engineer
was
operating in an unstimulating environment and attempting
to function at the lowest point of his circadian rhythm He may
have
awakened
from a microsleep spontaneously or
as
a result of
stimuli
Possible
stimuli
included
the sight and/or sound of the wig-wag signal, the sight and/or sound of train 891,
the
jolt
from the change in the roadbed as the train crossed the road crossing, or
the actions of other crewmembers
The
Safety
Board
believes
that the engineer failed to stop the train at the stop
signal
because
his chronic and acute fatigue32
caused
him to
fall
asleep for a critical
period of time.
Conductor of train 818 -The conductor quite likely suffered sleep deprivation
similar to that of the engineer. The conductor worked in
freight
pool service and
was
subject to the
same
irregularity and unpredictability of scheduling as was the
engineer.
His
last four tours of duty are illustrative.
Beginning
on November 4, he had
successive
starting times of 9 a m ,
2:45
a.m.,
4:30 a.m., and 10 15 p.m.
Thus,
he worked a day
shift,
two night shifts,
and
an evening
shift,
or changed
shift
twice in 4
days
His schedule encouraged
chronic
sleep
deprivation
He
did not suffer the short-term acute fatigue that the engineer did before
the accident
trip,
although the
Safety
Board
does not know what he did in Barstow
after he returned from eating with his crew. He may
have
slept, though he could
not
have
slept for more than 6 hours
However,
even
if
he
slept for those 6 hours,
he
would not
have
eliminated the
sleep
deficit
caused
by his
schedule.
When
the accident happened, he
was
working
during the low point of his circadian rhythm, He had no duties to perform, other
than that of being alert, once the train had entered the siding
Since
it is most
unlikely that the conductor would allow the train to
pass
the stop signal without
warning the engineer, the
Safety
Board
believes
that he too
was
asleep
as
the train
approached
the stop signal.
Brakeman
of train
818-She
had been working a fairly regular and
predictable schedule as a clerk before she became a brakeman, although her
schedule
changed while she was in brakeman
service.
She
did not experience the
^Dinges,
p 147
32Acute
fatigue
is
attributed
to
deficient
quality
and
quantity
of
sleep
within
one
normal
circadian
cycle
36
wide fluctuations in scheduling
that
the other two crewmembers did, thus, she
probably
was
not suffering from chronic sleep deprivation
The crew caller notified her at 8.43 p m., allowing her a
maximum
of
43 minutes of sleep before her
fateful
trip. Other than those possible 43 minutes,
her last bed rest was 26 hours 41 minutes before the accident. She had been in the
engineer's company all day until about 8 p.m., when she went to her motel room
On
the
trip
from Barstow she was probably tired enough to succumb to the
neurological pressures to sleep. As were the others, she was working during her
circadian
nadir. Her body was demanding sleep while she nevertheless had to be
awake.
Coupled with the neurological
pressures
were the facts
that
she was on the
return portion of her first road
trip
and she was unfamiliar with night operations,
with the Corona siding, and possibly with what to do in an emergency situation
Although she had been trained to be aware of stop
signals,
it is possible
that
since
this was her first
trip
at night, she overlooked the stop signal. Or, she may have
been reluctant to act on what she observed
The Safety
Board
concludes
that
either she was asleep due to acute fatigue,
did not know what to look for in unfamiliar territory at night, or was reluctant to
take action when train 818 passed the stop signal
Behavioral
Acti
ons
of the Crew of Train 818 —When a crewmember completes
a tour of duty, he usually goes to bed shortly after coming off duty because he
knows
that
in 8 hours he will be subject to being called for another tour He is
particularly likely to go to bed at an away-from-home terminal, where a layover is
usually
short However, sometimes a layover at an away-from-home terminal
exceeds
8 hours.
When
the crewmembers arrived in Barstow at 12'40 p m , both the engineer
and the conductor called their
wives
Each
estimated
that
he would not go back on
duty until about 5am the following day The estimates were based on the line-up
of trains and on the number of crews in Barstow at the time and on the fact
that
a
traincrew was normally called at 5 a m. The Barstow terminal had computer
monitors
that
crewmembers used to find out the train line-up and crew
information entered into
VIPS
According to the crew's estimates, they had enough
time to have a meal before they went to bed. After eating, the conductor followed
standard practice and went to his room
The engineer took a
different
approach to getting his rest. He stayed up,
intending (as he told his wife) to go to bed later in the day and sleep until he was
called
for work Had he been able to follow his plan, the time between the end of
his
sleep and the beginning of his tour of duty would have been minimal and he
would have been as well rested as possible In theory, his approach was sound. But
because
the unexpected occurred, in practice, it
was
not.
When
the crew arrived in Barstow and checked the line-up, it did not show
any
pending deadhead moves.
Based
on
that
information, the engineer's and
conductor's
estimates of their
next
duty times were reasonably accurate During
the day the engineer had conversations with members of other crews
that
were in
Barstow,
and they were not aware of any pending deadheads If the deadhead
information had been available earlier in the day, it might have been entered in
VIPS,
and the engineer might have made a
different
decision about when to go to
sleep.
Since
the information about the deadheading of crews was not available to
the engineer, he probably wanted to take his sleep at the time he had been
37
accustomed
to
during
the
previous
2
days,
which was
at
night
In
following this
course
of
action, he would have been better rested
at 5 a.m ,
when
he
expected
to
go on duty. He would have gone
to
bed about
8
hours before 5 am.
However,
he
should
not
have relied completely on
the
information from
VIPS
or from members
of
other
crews.
The carrier's employees knew
that
the scheduling
of trains and crews was subject
to
change Nevertheless,
the
Safety
Board
believes
that
the
carrier should more closely adhere
to the
schedule
for
posting updated
train and crew information every
4
hours.
Experience
should have tempered the engineer's reliance on
VIPS
Because
of
the weekly traffic
cycle
of
trains, crews were invariably deadheaded from Barstow
to
Los
Angeles
on
Tuesdays and sometimes
on
Wednesdays
The
engineer should
have
been aware
of
the need
to
check
VIPS
after
5
p.m. and should
not
have relied
on
information obtained earlier
that
day
However,
VIPS
was
not
updated every
4 hours,
in
this
case,
he would
not
have received the correct crew line-up until after
5-28 p m.
The Safety
Board
believes
that
had
the
ATSF
made
the
users
of
VIPS
aware
of
when
the
information had last been updated and when they could expect the
next
update,
it
might have made
a
difference. Had
the
above information about
the
deadheading
of
crews
out of
Barstow been available
at 1 p.m. or 5 p m.,
when
it
was
supposed
to
be,
the
crewmembers
of
train
818
might have made
a
different
decision
about how
to
spend their off-duty time
The Safety
Board
also concludes
that
the
engineer
was
imprudent
in not
trying
to
sleep during
the
off-duty time
that
the
carrier provided
in
compliance
with Federal regulations
The
carrier should
be
allowed, without running
the
risk
of contractual violation,
to
remove
an
employee from duty
if he
has admitted
to
not having enough sleep When
an
employee reports
that
he
is,
or is
reported
by
another employee
to
be, suffering from
a
lack
of
sleep,
a
procedure
is
needed
in
the crew calling system
that
allows him
to be
taken
out of
board rotation without
eitherthe carrier orthe employee incurring
a
penalty The procedure could work
in
a manner similar
to the
current by-pass agreement employed under rule
G
agreements
33
Acceptance
of
Work Assignment--Once
the
engineer learned
that
he was
being called
to
work
at 10:15 p.m ,
he complained
to
the crew caller about the fact
that
the three crews
in
front
of
him were being deadheaded He complained about
not getting his rest, and
he
implied
that
he
might
lay off
sick,
but he did not, and
he
accepted
the
call
He
continued his complaint
in a
conversation with
the
STO
and implied
that
he
had
not
slept during
the
day and was just getting ready
to go
to bed when he was called He told
the
STO,
". .I
mean
how
[do] you plan your
life, just live by
surprises?"
Had he chosen not
to
accept the assignment, he would have faced
at
least one
and perhaps as many as four
consequences.
The first would have been
the
loss
of a
33$everal
carriers
have
agreements with their respective labor organizations about the handling of an
employee
who has had an alcoholic
beverage
while on call If the employee admits to having had the
beverage,
he is by-passed from duty and dropped to the bottom of the call board No penalty is
incurred by eitherthe employee or the carrier
38
tour of duty and no compensation The second was
that
he would have had to
provide his own transportation home; the carrier would not furnish such
transportation. The latter have would been of
little
consequence since he coowned
an automobile
that
was garaged in Barstow.
A
third consequence might have been peer pressure from the other
crewmembers. The remainder of the crew could have been deadheaded home, or
it could have had another engineer assigned and taken the trip. If the
crewmembers were deadheaded, their pay would have been
less
than if they
worked a train to Hobart yard.
A
fourth consequence
that
might have affected the engineer's decision was
the prospect of disciplinary action. The regional manager said ".. [if the engineer]
didn't have a history of it [laying off], and even though if it wasn't perceived as a
good reason, I'm confident there wouldn't have been any punitive measures
taken .." However, disciplinary action was a possibility because the engineer had
laid off twice on call and the
ATSF
had not taken any action either time. He might
have
believed
that
another lay-off on call would have prompted action by the
carrier
During his testimony to the Safety
Board,
the STO expressed "sympathy" for
the engineer's predicament but said
that
when he had too many crews for the
trains available, as he did in this
case,
he had to deadhead. He said the engineer's
situation had never come up before, nor was he aware of anyone ever having laid
off at an away-from-home terminal because he was tired The carrier had not
provided policy guidance on what to do when a crewmember notified the STO of
not having slept prior to coming on duty. Thus, no precedent seems to have been
established on the
ATSF
for treating sleepiness in the same manner as other sources
of impairment.
The Safety
Board
believes
that
outside pressure (personal commitment, peers,
and professionalism) and circumstances (being at an away from home terminal)
weighed heavily in the engineer's decision to accept the assignment. Despite his
fatigue and lack of sleep, he believed
that
his best recourse was to take the
assignment
As
a result of the Safety
Board's
investigation of the collision between two
Consolidated Railroad Corporation freight trains at Thompsonstown, Pennsylvania,
the following recommendations were addressed to the AAR pertaining to
work/rest
cycles
and performance of personnel on March
30,1989:
R-89-21
Encourage
its member railroads to improve their current
methods of using train crews to reduce the irregularity and
unpredictability of their work/rest
cycles.
R-89-22
Encourage
member railroads to provide education and
counseling to employees on proper health regimens and
avoidance
of sleep deprivation.
39
R-89-23
Recommend
to
those member railroads with locomotive
cab
signal
systems
to
evaluate their
cab
signal acknowledging
devices
and
redesign those
that
could
be
operated through
a
simple motor response by a sleeping engineer
The AAR responded
on
October
12, 1989,
citing numerous ongoing activities
by various railroads
to
correct problems associated with improper work/rest
cycles.
The Safety
Board
replied
by
asking
the
AAR
to
take
an
active role
in
encouraging
member railroads
to
adopt policies and programs related
to
proper work/rest
cycles
and health regimens.
The
AAR,
at a
meeting with Safety
Board
staff
in May 1991,
stated
that
another
effort
would
be
made by
the
association
to
make
the
industry
more aware
of
this issue Meanwhile, these safety recommendations
are
being
held
in an
"Open-Acceptable
Response"
status pending
the
completion
of the
described
efforts.
The Safety
Board
has made several intermodal recommendations concerning
the study
of
work/rest
cycles
and performance
of
personnel.
On May 12, 1989, the
Safety
Board
issued three safety recommendations
to the
Secretary
of the
Department
of
Transportation
(DOT)
related
to
human fatigue
in
transportation.
These
safety recommendations are
1-89-1
Expedite
a
coordinated research program
on the
effects
of
fatigue sleepiness, sleep disorders,
and
circadian factors
on
transportation system safety
1-89-2
Develop
and
disseminate educational material
for
transportation industry personnel and management regarding
shift work, work
and
rest schedules;
and
proper regimens
of
health,
diet, and rest
I-89-3
Review
and upgrade regulations governing hours
of
service
for
all transportation modes
to
assure
that
they are consistent and
that
they incorporate
the
results
of the
latest research
on
fatigue and sleep
issues.
These
Safety Recommendations
are a
part
of the
Safety
Board's
"Most
Wanted
Safety Recommendations Program
"
The
DOT
responded
on
August
11, 1989,
citing ongoing human factors
research
in the
various modal administrations
of DOT, the DOT
Research
and
Development Coordinating Council,
the
then-proposed
DOT
National
Transportation
Policy
statement,
and
ongoing reviews
of
policy regarding
dissemination
of
educational materials
and
hours-of-service regulations
in the
various
modal administrations
The
Secretary advised
that
he
would keep
the
Safety
Board
apprised
of
progress.
40
On
September
12,1990,
officials from the DOT pointed out at a meeting with
Safety
Board
staff
that
the DOT was supervising a comprehensive program of
research
on human factors in transportation, including the
causes
of transportation
accidents,
the effects of operator impairment, perceptual errors, and fatigue, as
well
as design and operating changes
that
can eliminate or reduce those effects
Each
of the modal administrations
discussed
ongoing efforts related to this issue
and
how the individual efforts fit into the overall DOT policy
The
FRA reported on the work being carried out in the railroad industry to
document the performance of railroad engineers. The FRA is also conducting
interviews
with workers in the industry in an
attempt
to determine the actual
extent
of any operator overwork issue From these interviews, the
FRA
will
attempt
to sort out
issues
such
as:
o
reasonable commuting
distances
for operating personnel,
o
potential needed
revisions
to the Hours of
Service
Act, and
o
other efforts
that
may be needed to bring about a more
normal work environment for rail crews
The
Safety
Board
realizes
that
this kind of
effort
will require time to complete.
On
June
21, 1991, the Chairman of the National Transportation Safety
Board
addressed
Congress
and noted the following pertaining to work/rest
cycles.
We
are aware
that
the Federal Railroad Administration (FRA) is
conducting
industry interviews in an
attempt
to determine the
true
extent
of the work/rest problem. They will
attempt
to
determine what a reasonable commuting distance is for
locomotive
crews and what other
changes
might be needed to
bring about a more normal work environment for rail crews
However,
it must be recognized
that
the ability of the FRA to
do anything about these
issues
has been impeded, since the
work hours of railroad employees-unlike those in any other
mode of transportation-are governed by the Hours of
Service
Act
(Act). While
Congress
had made some minor modifications
to this law, it has remained essentially unchanged since it was
signed
into law by President Theodore Roosevelt in 1907
Ultimately, action by Congress will be needed to address key
issues
relating to the Act Most importantly, we believe the
FRA
should have the ability to work within the Act, so
that
regulations stemming from the Act can change as the times
change.
In
that
way, the FRA could mandate breaks and
off-duty periods for train dispatchers and operators, and new
workload limits for train dispatchers could be determined,
without an act of
Congress
Positive
Train Separation
Notwithstanding the failure of the crewmembers of train 818 to comply with
the stop signal on the west end of the Corona siding, the accident probably would
have
been prevented had the carrier been using a positive train separation system.
41
A
properly designed and functioning system would have stopped the train before it
passed
the stop signal. The Safety
Board
realizes
that
much work remains to be
done before a complete positive train separation system can be implemented.
Nonetheless,
this is another collision
that
could have been averted had a positive
train separation system been available The Safety
Board
recently investigated a
collision
on the Norfolk Southern Railway at Sugar Valley, Georgia, and on the
Southern
Pacific
Railroad near Tucson, Arizona, in which the circumstances were
similar to those in this accident
If an
ATCS
had been monitoring the location, speed, and handling of train
818, the dispatch computer would have recognized the fluctuation in speed from
San
Bernardino to Corona and the engineer's failure to take action to brake as the
train moved closer to the stop signal. Through a data radio link, the dispatch
computer would have stopped train 818, thereby avoiding the collision. The
railroad industry and the FRA must expedite the development of positive train
separation systems
As
a result of the Sugar Valley accident, the Safety
Board
on
July
9, 1991,
recommended to the FRA
1
In conjunction with the Association of American Railroads and
the Railway Progress Institute, expand the
effort
now being
made to develop and install advanced train systems for the
purpose of positive train separation
Pathological
The autopsy surgeon reported the cause of death of all three crewmembers of
train 818 to be smoke inhalation and thermal burns The report noted "soot in the
airways";
however, the autopsy reports were limited in descriptive information
For
example, the depth of smoke inhalation in the respiratory tract was not
provided In addition to the soot inhalation observations, one autopsy report
referred to the "cherry red blood, carbon monoxide intoxication" in one of the
smoke inhalation victims The toxicology reports did not reflect elevated COHb, as
would be expected from death due to smoke inhalation
There are two possible explanations for the absence of elevated COHb in the
smoke inhalation victims The most likely reason for the negative COHb finding is
the inappropriate analysis for carbon monoxide
Because
the information
concerning
the nature of the specimens was unknown to the toxicologist, the
laboratory used a spectrometric analytical procedure. However, because the
victims
were severely burned, it is highly probable
that
methemogiobin was also
elevated,
which can result in interference with carboxyhemoglobin analysis.
The second possible reason for the absence of elevated COHb is the reported
postaccident flash fire
that
occurred. This flash fire could have led to rapid death,
which
could have prevented the development of elevated carboxyhemoglobin
However,
this latter rationale is unlikely since the autopsy report indicated cherry
red blood in one victim, which is an unusually reliable symptom of elevated
carboxyhemoglobin saturation Therefore, the Safety
Board
concludes
that
the
crewmembers on
ATSF
818 died due to smoke inhalation and thermal burns
42
Drug Issue
Conductor of train 891 .-That his urine showed traces of morphine and his
blood did not is consistent with his having received morphine about 4 1/2 hours
before the specimens were collected. He was given morphine to help him cope
with the pain caused by the injuries he received in the accident
Engineer
of train 891 .--His urine, which was positive for amphetamines
(stimulants), also indicated a low concentration of the carboxylic acid metabolite of
marijuana These findings are consistent with the engineer's previous drug testing
history. Although the drug counselors determined
that
the engineer of train 891
did not have a chemical dependency problem, the engineer failed three drug tests
during a period of about 20 months There is no evidence
that
the engineer knew
that
he was being drug tested when he took the physical
that
indicated he was
positive for THC and methamphetamine. However, the drug tests
that
the
engineer subsequently failed were, for all practical purposes, announced because
he was notified by certified letters from Chicago and did not pick up these letters
for an extended period of time. According to medical department rules, with
which
he complied, he was required to provide a urine specimen within 5 days of
receipt of notification.
This record supports the conclusion
that
the engineer refrained from using
drugs long enough to pass repeat tests The presence of the inhaler containing
metnamphetamine in his bag suggests
that
he was using the drug on the job The
inhaler was not the type used for an over-the-counter inhaler containing the
decongestant isomer of methamphetamine; it was most probably obtained for
illicit drug use.
Because
the drug was not detected in his blood, he probably had
not used it on the day of the accident (although detection in the blood depends
greatly on the amount used because the half life is 12 to 34 hours, depending on
urine pH). He provided a drug testing specimen about
11
hours after the accident.
The presence of the stimulants methamphetamine and amphetamine and the
presence
of the acid metabolite of the hallucinogen marijuana in the engineer's
urine are consistent with his continued use of these drugs. The engineer supplied a
final urine specimen for drug testing on March 23, 1990, and this specimen was
negative for the five drugs required in the DOT drug testing program. However,
this specimen had been required after he had submitted a positive specimen on
December 22, 1988, and he delayed providing a specimen at
that
time for more
than 30
days.
This accident occurred about 7 months after the last "unannounced" drug
testing of the engineer The presence of 8 ng/ml of marijuana metabolite in his
urine suggests
that
he continued his use of marijuana between the last testing and
the accident He continued to use the stimulant methamphetamine and, in fact,
carried methamphetamine, an addictive drug, with him on the train
Methamphetamine is a central nervous system stimulant, producing effects
similar to
that
of cocaine, except the effects of methamphetamine last longer. The
engineer was probably taking the drug to enhance his alertness, or to try to
compensate for lack of proper rest However, there is no concrete evidence
that
performance is enhanced. Studies have shown
that
the drug has disruptive effects
on behavior and leads to more aggressive behavior. Continued use leads to
psychosis
that
includes symptoms of
persecution,
hyperactivity, visual and auditory
43
hallucinations,
and change in body image Increased aggressive behavior is likely to
lead to increased risk taking and aggressive train operations
The
FRA's
regulation (49 CFR Part 219) did not explicitly provide guidance on
the finding of illegal substances during an employee's annual physical However,
the
ATSF
issued its own policy, under which the medical department did not divulge
the results of a drug test to other departments if the test was taken as part of a
routine physical Consequently, although the medical department knew about the
engineer's positive test
results,
the operations department did not.
The results of the
ATSF
follow-up and the Federally required postaccident
testing indicate
that
the engineer was a chronic user of the stimulant
methamphetamine and of tetrahydrocannabinol (marijuana). This drug use
pattern suggests
that
he had a continuing drug problem
that
was not recognized as
such
by the
EAP
counselor. The engineer simply stopped using drugs each time he
failed a drug test and then refrained from taking any until he was able to pass a
retest
The Safety
Board
is concerned about the use and abuse of drugs by any
railroad employee However, the Safety
Board
is especially concerned
that
this
individual was not removed from his safety-sensitive position when he had been
identified in repeated tests
as
a drug user 2 years earlier.
Examination of the engineer's record shows
that
ATSF's
former drug policy
was
seriously flawed, it allowed the engineer to continue to operate despite his
repeated use of drugs The new
ATSF
drug policy has addressed this issue by
directing
that
each employee be allowed only one positive test result for drug use.
If a second incident should occur, the employee will be terminated from
employment by the carrier. The Safety
Board
recognizes the
ATSF's
efforts and
initiative in addressing the issue of drug use by its employees
Work
Records
Although the
ATSF
was in complete compliance with the maintenance of
hours-of-service
records as specified by 49 CFR subpart 228 11, investigators had
trouble deciphering the information in these records pertaining to the work/rest
cycles
of the engineer on train 818 The
ATSF
developed its own record keeping
system
because there were no Federal guidelines to assist carriers in providing and
maintaining the information
As
the importance of tracking work/rest
cycles
grows
within the rail industry, so will the importance of the
format
used in recording the
necessary
information. The Safety
Board
believes
that
a simple
format
should be
designed by the
FRA
so
that
it
is
easier to follow hours-of-service information
Locomotive
Crashworthiness
The Safety
Board
believes
that
the majority of the damage sustained by the
lead locomotive of train 818 was the result of the accident dynamics
that
occurred
subsequent to the initial impact, No survivable space was
left
in the control
compartment as a result of the initial impact However, the bulk of the damage to
the conventional cab of this unit was caused when train 891's third locomotive
came
to rest on top of its control compartment.
44
Because
the trains initially collided somewhat off center (left
front
to
left
front), the collision was not directly "head on," and the crash-resistant systems on
train 818's lead locomotive unit were not fully
utilized
Thus, this accident did not
provide a full assessment of how the North American cab would react in a direct
head-on collision Due to the closeness in sill heights of the two lead locomotive
units,
there was no override in this accident.
The North American cab did perform its intended function, offering
survivable
space in a collision despite the death incurred by a crewmember riding in
one of these compartments. However, the Safety
Board
was unable to compare the
crashworthiness of the North American cab in this accident to its crashworthiness in
other collisions due to the lack of data collected by the FRA The database of the
FRA
data collection system does not specifically address the locomotive unit type
involved in an accident.
Train 891's lead locomotive had not sustained any fire damage, however, its
second
and third locomotives were extensively burned The structural integrity of
the control compartments of all three locomotives remained intact, maintaining
survivable
space for all occupants. Although the locomotives separated and
derailed in the accident, the most serious damage they sustained was caused by the
fire. The Safety
Board
believes
that
this collision did not yield adequate
information to evaluate the crashworthiness of the
EMD-GP
60M
Fuel
Tank Crashworthiness
Due to the lack of data, the Safety
Board
could not analyze the prevalence of
fuel-tank-induced fires in rail collisions The FRA data collection system does not
specifically address the
matter
of fuel tank involvement in accidents
The Safety
Board
is concerned
that
diesel fuel-generated fires can trap and
burn crewmembers and cargo, contribute to starting hazardous-materials fires in
the train, and place nonrailroad property in harm's way. Of the 643 rail accidents
that
have been investigated by the Safety
Board,
23 had damaged locomotive fuel
tanks
that
resulted in fire The Safety
Board
believes
that
there
is
a need to analyze
the location and protection of the locomotive fuel tanks Thus, more information is
needed concerning accidents
that
involve damaged fuel tanks.
Consequently, the Safety
Board
believes
that
the FRA needs to revise its data
collection procedures so
that
it can identify the kinds of units
that
are involved in
accidents,
the accidents
that
involve fires, and the accidents in which the fuel tanks
are ruptured.
Event
Recorders
The fire destroyed the event recorders on the second and third units on train
891 An inspection of the fire-damaged units showed
that
the location of the
recording equipment provided satisfactory protection from crash forces. However,
the type of encasement employed by the manufacturer did not provide adequate
thermal protection Had there been an event recorder on the lead unit,
information would have survived the collision because the control department of
the unit did not sustain any fire damage.
45
The most feasible approach to the preservation of event recorders is to set
standards
for resistance to crash forces and fire for these
devices.
The Safety
Board
believes
that
the FRA needs to develop requirements for
crash-
and fire-resistant
event recorders similar to those used in aircraft Further, the
Board
believes the
FRA
should require event recorders on all locomotives.
Although the FRA recognized the need for more durable encased event
recorders
in its notice of proposed rulemaking
(NPRM)
dated
June
19, 1991, the
rulemaking does not require event recorders on all locomotives. The Safety
Board
will address both
issues
in its comments on the rulemaking
Notification of Pipeline Operators
The Safety
Board
recognizes the
effort
that
the
ATSF
made to maintain a list
of telephone numbers of those who should be notified when an accident occurs
However,
the list used in this accident did not include the names or phone numbers
of the operators of the two pipelines
that
were in the vicinity of the accident site.
In California, the natural gas pipeline operators were under the jurisdiction of
the California Public Utilities Commission
(CALPUC),
and the petroleum pipeline
operators were under the jurisdiction of the California State Fire Marshal's Office.
Both
agencies had listings of their operators, but had not provided this information
to the
ATSF
When the accident happened,
CALPUC
was in the process of compiling
a list of operators whose pipelines ran parallel to or
crossed
railroad rights of way
Previous
pipeline accidents have demonstrated how catastrophic such
accidents
can be Considering the potential for an accident in Corona, the Safety
Board
believes
that
when a rail accident
occurs,
there is an urgent need to notify
pipeline operators of pipelines
that
may be affected. The pipeline operators,
governing agencies, and the rail carriers should work together to devise an efficient
notification process.
CONCLUSIONS
Findings
1
No anomalies or deficiencies were evident in the train brakes of either freight
train or in the track or signal
systems
that
contributed to the accident.
2
The engineer of train 818 failed to stop his train on the Corona siding at the
stop signal because he was asleep or in a microsleep brought about by chronic
and acute fatigue.
3. The chronic and acute fatigue of the engineer of train 818 was a result of the
irregularity and unpredictability of
his
work schedule.
4.
Because
of fatigue, the conductor of train 818 either was asleep or
experienced a microsleep as his train approached the stop signal on the west
end of the Corona siding.
5
The brakeman of train 818 failed to take action to stop the train probably
because
she fell asleep as a result of acute fatigue.
46
6. The Atchison, Topeka and Santa Fe Railway Company did not have a policy or
procedure in place to address the issue of an employee notifying the carrier of
his
or her lack of sufficient sleep
7. When the engineer of train 891 saw the 2R signal at Corona suddenly turn
red,
it was too late to take action to avert the accident.
8. Although the urine sample of train 891's engineer had traces of drugs, it could
not be determined whether the drugs impaired his performance at the time
of the accident. His actions did not contribute to the accident.
9 The Atchison Topeka and Santa Fe Railway Company policy of using certified
letters to announce random drug screens was ineffective because it allowed
the recipient of the letter to delay accepting the
letter,
thereby avoiding
timely testing.
10. The encasements used to hold the event recorders
that
were on train 891 did
not protect the recorders from fire damage Thus information about the
handling of train 891 was incomplete
11 Neither research nor accident data exist about the effect of ruptured or
leaking locomotive fuel tanks in railroad accidents in which postcrash fires
occurred
12 The Atchison Topeka and Santa Fe Railway Company accident notification
process
did not include the emergency
24-hour
telephone numbers of
operators of pipelines
that
might have been affected by an accident
13 The accident probably would have been prevented had the trains been
separated by a fully implemented advanced train control system,
Probable
Cause
The National Transportation Safety
Board
determines
that
the probable cause
of the collision was the failure of the engineer of train 818 to stop his train at the
stop signal because he was asleep. Contributing to the accident was the failure of
the conductor and the brakeman to take action, probably because they too were
asleep,
to stop the train. Also contributing to the accident were the irregular
unpredictable work schedule of the engineer on train 818, the Atchison, Topeka and
Santa
Fe Railway Company's lack of a policy or procedure for removing
crewmembers from service when they are not fit for duty because of a lack of sleep,
and the inadequacy of the Federal rules and regulations
that
govern hours-of-
service
RECOMMENDATIONS
As
a result of its investigation, the National Transportation Safety
Board
recommends
-to the Federal Railroad Administration.
Develop a uniform simplified
format
for work-record data
collected by the rait carriers,
(Class
II, Priority Action)
(R-91-39)
47
To enhance current accident data collection and analysis,
require the recording of data pertaining to postcrash fires
involving locomotive fuel tank rupture and spillage, as well as
types
of locomotive units involved.
(Class
II, Priority Action)
(R-91-40)
--to the Atchison Topeka and Santa Fe Railway Company:
In cooperation with the operating unions, develop an
educational and counseling program designed to improve
crewmembers' knowledge of health and diet regimens and
methods of avoiding sleep deficits and sleep deprivation
(Class
II, Priority Action)
(R-91-41)
In cooperation with the Association of American Railroads and
the operating unions, develop a policy
that
would allow the
carrier to stop an employee from accepting assignments and
that
would allow an employee to report off duty when the
employee is impaired by lack of sleep.
(Class
II, Priority Action)
(R-91-42)
Post
on the Voice Information Processing System and on all
crew
call monitors the time of the last update and of the
next
projected update.
(Class
II, Priority Action)
(R-91-43)
In cooperation with the California Public Utilities Commission
and the California State Fire Marshal's Office, develop a
complete list of
24-hour
emergency telephone numbers for
those pipeline operators whose transmission lines are near the
Atchison,
Topeka and Santa Fe Railway property.
(Class
II,
Priority Action)
(R-91-44)
-to the Association of American Railroads:
In cooperation with member carriers and the operating unions,
develop a policy
that
would allow the carrier to prevent an
employee from accepting assignments and would allow an
employee to report off duty when he or she is impaired by lack
of
sleep.
(Class
II, Priority Action)
(R-91-45)
In cooperation with member carriers and the Federal Railroad
Administration, develop a uniform simplified
format
for
work-record data collected by the rail carriers.
(Class
II, Priority
Action)
(R-91-46)
-to the Brotherhood of Locomotive Engineers
In cooperation with all rail carriers, develop a policy
that
would
allow the carrier to prevent an employee from accepting
assignments and would allow an employee to report off duty
when he or she is impaired by lack of sleep
(Class
II, Priority
Action)
(R-91-47)
48
to the United Transportation Union:
In cooperation with all rail
carriers,
develop a policy
that
would
allow the carrier to prevent an employee
from
accepting
assignments
and would allow an employee to
report
off duty
when he or she is impaired by lack of sleep
(Class
II, Priority
Action)
(R-91-48)
-to the California Public Utilities Commission
In cooperation with the
Atchison,
Topeka and Santa Fe Railway
Corporation
(ATSF)
and the California State Fire Marshal's
Office,
develop a complete list of
24-hour
emergency phone
numbers for those pipeline operators whose transmission lines
are
near
ATSF
property.
(Class
II, Priority Action)
(R-91-49)
-to the California State Fire Marshal's Office*
In cooperation with the
Atchison,
Topeka and Santa Fe Railway
Corporation and the California Public Utilities Commission,
develop a complete list of
24-hour
emergency telephone
numbers of those pipeline operators whose transmission lines
are
near
ATSF
property
(Class
II, Priority Action)
(R-91-50)
BY
THE NATIONAL
TRANSPORTATION
SAFETY
BOARD
Isl
James
L. Kolstad
Chairman
/s/
Susan
M. Couqhlin
Vice
Chairman
Is/
John
K. Lauber
Member
Isl
Christopher A. Hart
Member
/si
John
A. Hammerschmidt
Member
July
23, 1991
49
APPENDIXES
APPENDIX
A
INVESTIGATION
AND
HEARING
Investigation
The Safety Board was notified of the accident at 9 a.m. on November 7, 1990,
and immediately dispatched an investigator from the Denver field office to the
scene
The Safety Board Chairman, a Member, the Managing Director, the Director
of the Office of Surface Transportation Safety, the investigator-in-charge, and
other members of the investigative team were also dispatched from Washington,
D C. Investigative groups were established for operational, track, signal, human
performance, and survival factors
Hearing
The Safety Board convened a
2-day
deposition hearing as part of its
investigation on
January
21, 1991, at Riverside, California Parties to the hearing
included the
Atchison,
Topeka and Santa Fe Railway Company, the Federal Railroad
Administration, the General Motors Electro-Motive Division, the Brotherhood of
Locomotive
Engineers, the State of California Public Utilities Commission, and the
United Transportation Union
51
APPENDIX
B
PERSONNEL
DATA
ATSF818
Engineer
Mr. Gary R Ledoux, 35, had been hired by the AT5F as a clerk on August 27,
1973. In 1978 he accepted a position as a fireman and was promoted to engineer
on February 26, 1980 The engineer's most recent training was in 1989, when he
attended a locomotive operations seminar He successfully completed his last rules
class
on February
27,1990
According to carrier records for the period from
January
1989 through October 1990, he was given 76 efficiency tests with no failures.
Conductor
Mr
James
S.
Wakefield, 55, had been hired by the
ATSF
on May 10, 1956, as a
brakeman On May 1, 1961, he was promoted to conductor in the San Bernardino
subdivision and worked his entire career in this area His most recent training
occurred on April 11, 1989, when he attended a periodic ATSF-sponsored
conductor's training
class.
His last rules
class
was on
June
28, 1990 According to
carrier records for the period from
January
1989 through October 1990, the
conductor was given 24 efficiency tests with one failure, which occurred on
August
1,1990
Brakeman
Ms
Virginia C Hartzell, 29, had been hired by the
ATSF
police department on
June
1,1981,
as a clerk On November
16,1989,
she changed positions and became
a dispatcher trainee in San Bernardino She was promoted to dispatcher on May 1
1990, and
left
the dispatcher's office on August 30, 1990, to be a clerk in Hobart
yard until transferring to the operating department as a brakeman on October 22,
1990 On November 2, 1990, she was placed on the brakeman's
extra
board. Her
most recent training was a brakeman-in-training course from October 22 through
November 1, 1990 No records indicate
that
she had taken any rules examinations
or efficiency tests since she became a brakeman. Records indicate
that
she did
pass,
with a high
score,
the stringent dispatcher's examination and also passed the
switchman's examination. According to company records, no disciplinary action
was
taken against her during her tenure with the carrier
ATSF
891
Engineer
Mr
James
A. Dawson, 50, had been hired by the
ATSF
on
July
9, 1971, as a
chair car attendant in Los Angeles. He held this position until September 9, 1971,
when he transferred to the operating department as a switchman On November
11,
1971, he
left
the operating department and became a clerk in the Los Angeles
division He held this position until transferring to fireman's status on
July
25,1974,
and was promoted to engineer on February 13, 1976, in the Los Angeles division.
He successfully completed his last rules
class
on
June
11, 1990. According to carrier
records
for the period from
January
1989 through October 1990, he was given
36 efficiency tests with 3 failures.
53
APPENDIX
C
RULES
APPLICABLE
TO THIS
REPORT
This report refers to several rules listed in the General Code of Operating
Rules,
which are quoted here in full:
RuleG
The use of alcoholic beverages, intoxicants, drugs, narcotics,
marijuana or controlled substances by employees subject to
duty, when on duty or on Company property is prohibited
Employees
must not report for duty or be on Company
property under the influence of or use while on duty or have
in their possession while on Company property, any drug,
alcoholic
beverage, intoxicant, narcotic, marijuana,
medication, or other
substance,
including those prescribed by
a doctor,
that
will in any way adversely affect their alertness,
coordination, reaction, response or safety
Rule
34 Observe and Call
Signals:
Crewmembers in control
compartment of engine must be alert for and communicate
to each other in a clear and audible manner, the name or
aspect
of each signal affecting the movement of their train as
soon
as it becomes visible or audible They must continue to
observe
signals and call any change of aspect until passed
If prompt action is not taken to respect signal, other
crewmembers must remind engineer and/or conductor of rule
requirement, and if no response, or engineer is incapacitated,
other crewmembers must take immediate action to ensure
safety, using emergency brake valve to stop the train if
necessary.
Rule
89 Stopping Clear: A train stopping where it may be met or
passed
must stop and remain not
less
than 400 feet from the
signal or clearance point of facing point switch over which a
train may
pass,
if length permits
Rule
620 Riding Engine: When practicable, crewmembers on head-end
of freight trains must ride in control compartment of the
engine When the conductor is riding the head-end, he will
ride in the control compartment.
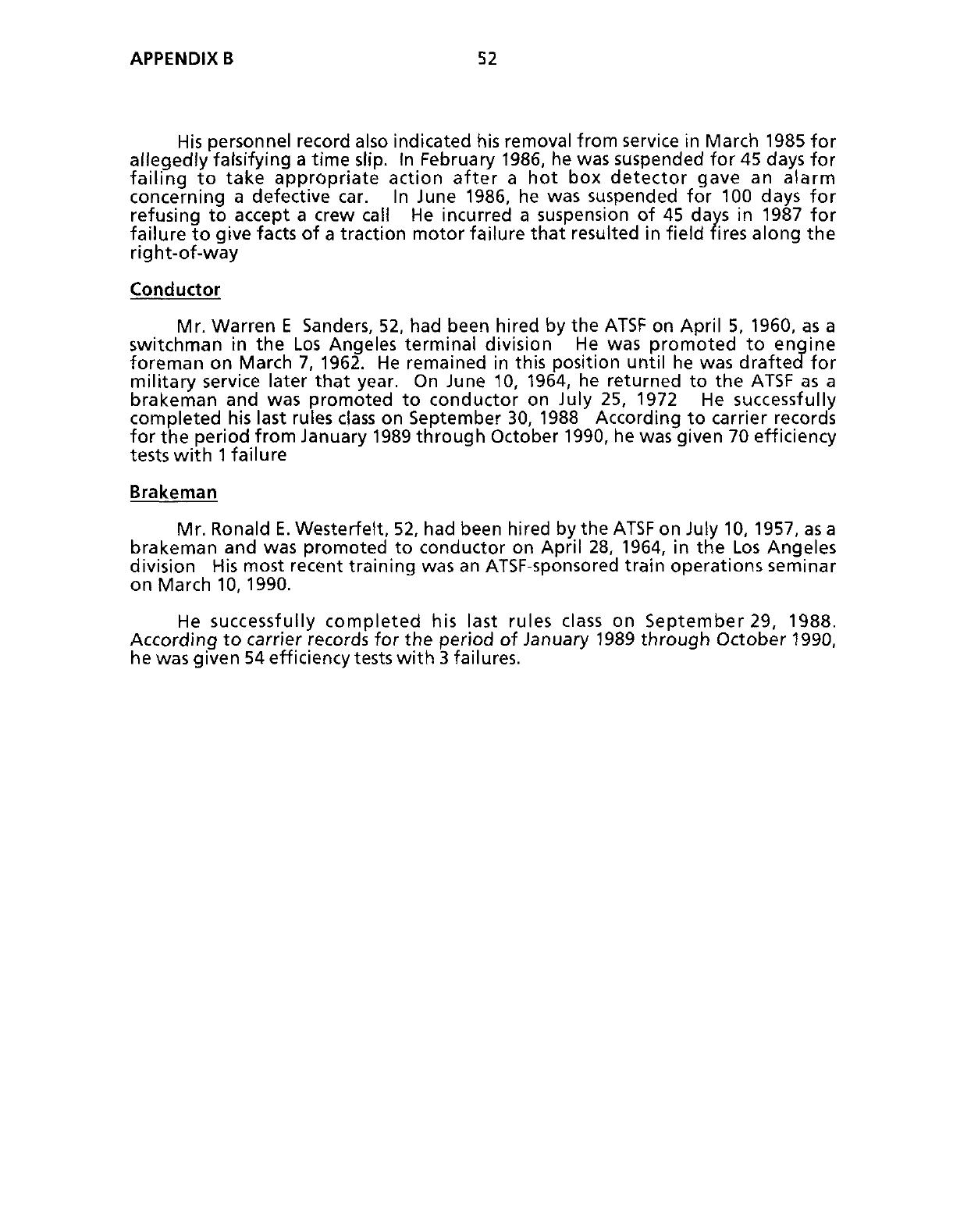
APPENDIX
B 52
His
personnel record also indicated his removal from service in March 1985 for
allegedly falsifying a time slip. In February 1986, he was suspended for 45 days for
failing to take appropriate action after a hot box detector gave an alarm
concerning a defective car. In
June
1986, he was suspended for 100 days for
refusing to accept a crew call He incurred a suspension of 45 days in 1987 for
failure to give facts of a traction motor failure that resulted in field fires along the
right-of-way
Conductor
Mr. Warren E
Sanders,
52, had been hired by the
ATSF
on April 5, 1960, as a
switchman in the Los Angeles terminal division He was promoted to engine
foreman on March 7, 1962. He remained in this position until he was drafted for
military service later that year. On
June
10, 1964, he returned to the
ATSF
as a
brakeman and was promoted to conductor on
July
25, 1972 He successfully
completed his last rules
class
on September 30, 1988 According to carrier records
for the period from
January
1989 through October 1990, he was given 70 efficiency
tests
with
1
failure
Brakeman
Mr. Ronald E. Westerfett, 52, had been hired by the
ATSF
on
July
10, 1957, as a
brakeman and was promoted to conductor on April 28, 1964, in the Los Angeles
division
His most recent training was an
ATSF-sponsored
train operations seminar
on March
10,1990.
He
successfully completed his last rules
class
on September 29, 1988.
According
to carrier records for the period of )anuary 1989 through October 1990,
he
was given 54 efficiency tests with 3 failures.
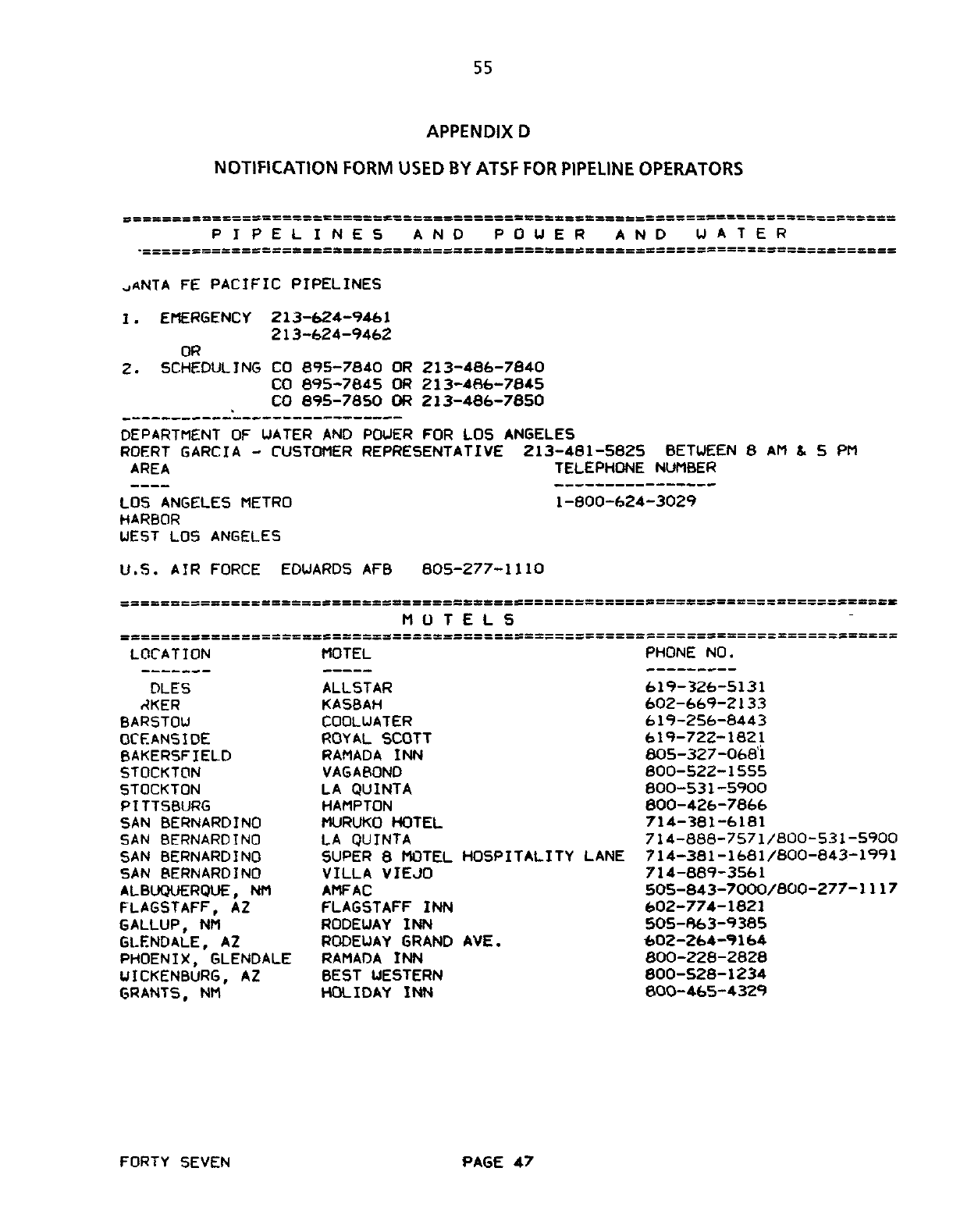
55
APPENDIX
D
SSSSSSSS====
=
SSE=SS«S=S£SSSS===SSSSSSSSBSSSSSKXSaSSSSSS==SSSS==S=SUsSSSSSSS
PIPELINES
AND
POUER
AND
WATER
uANTA
FE
PACIFIC PIPELINES
1. EMERGENCY 213-624-9461
213-624-9462
OR
2. SCHEDULING
CO
895-784.0
OR
213-486-7840
CO 695-7845
OR
213-466-7845
CO 895-7850
OR
213-486-7850
DEPARTMENT
OF
UATER
AND
POUER
FOR LOS
ANGELES
ROERT GARCIA
-
CUSTOMER REPRESENTATIVE 213-481-5825 BETWEEN
8 AM S. 5 PM
AREA TELEPHONE NUMBER
LOS ANGELES METRO
HARBOR
UEST
LOS
ANGELES
U.S.
AIR
FORCE EDUARDS
AFB
805-277-1110
1-800-624-3029
MOTELS
LOCATION
DLES
AKER
BARSTOW
OCEANSIDE
BAKERSFIELD
STOCKTON
5T0CKT0N
PITTSBURG
SAN
BERNARDINO
SAN
BERNARDINO
SAN
BERNARDINO
SAN
BERNARDINO
ALBUQUERQUE,
NM
FLAGSTAFF,
AZ
GALLUP,
NM
GLENDALE,
AZ
PHOENIX, GLENDALE
UICKENBURG,
AZ
GRANTS,
NM
MOTEL
ALLSTAR
KASBAH
COOLUATER
ROYAL
SCOTT
RAMADA
INN
VAGABOND
LA
QUINTA
HAMPTON
MURUKO HOTEL
LA
QUINTA
SUPER
8
MOTEL HOSPITALITY LANE
VILLA VIEJO
AMFAC
FLAGSTAFF
INN
RODEUAY
INN
RODEUAY GRAND
AVE.
RAMADA
INN
BEST WESTERN
HOLIDAY
INN
PHONE
NO.
619-326-5131
602-669-2133
619-256-8443
619-722-1821
805-327-0681
600-522-1555
800-531-5900
800-426-7866
714-381-6181
714-888-7571/800-531-5900
714-381-1681/800-843-1991
714-889-3561
505-843-7000/800-277-1117
602-774-1821
505-863-9385
602-264-9164
800-228-2828
800-528-1234
800-465-4329
FORTY SEVEN
PAGE
47
NOTIFICATION
FORM
USED
BY
ATSF
FOR
PIPELINE
OPERATORS
57
APPENDIX E
ATSF DRUG POLICY
APPENDIX
E
58
TO
ALL EMPLOYEES:
The object of
this
policy statement is to (I)
provide a safe and efficient work environment
for employees, and
(2)
encourage troubled em-
ployees to take advantage of
the
programs out-
lined herein Santa Fe employees must be free
from the effects of alcohol or drug use on the
job We must all recognize that a serious
problem exists and identify employees who
can be helped through counseling and rehabili-
tation. Treatable problems should not be al-
lowed
to
become progressively worse and lead
to resolution by disciplinary action.
You are encouraged to review this policy
statement and keep its provisions in mind.
While recourse to disciplinary measures can-
not be completely eliminated, voluntary refer-
ral and co-worker reports offer employees
better
alternatives.
The interests of employees
and their families, the public and the company
are best served by controlling personal prob-
lems arising from the use of alcohol and drugs
that interfere with health, work, and safety.
I sincerely solicit your enthusiastic cooper-
ation and interest in complying with this
policy.
M. R. Haverty
President
The Atchison, Topeka and
Santa Fe Railway Company
Chicago, Illinois
59
APPENDIX
E
Policy
on Use of
Alcohol
and
Drugs
by
Employees
of
THE
ATCHISON,
TOPEKA
AND
SANTA
FE
RAILWAY
COMPANY
1
0 OBJECTIVE
The
Atchison,
Topeka and
Santa
Fe
Railway
Company
(Santa
Fe)
strives to
contribute
to
the
health
and
well-being
of
employees
by
providing
a
safe
and
efficient work environment
A work-
place
which
is
free
from
the
effects
of
alcohol
and
drugs
is
necessary
to
accomplish
this
goal
This
policy is
designed to
protect
our
employees
and
the
public
from
the
undesirable
consequences
of
allowing
the
employment
of
any
individual
whose
actions
may
be
influenced
or
impaired
by
the use
of
alcohol
or
drugs
Santa
Fe
endorses
and
complies with
regula-
tions covering this
subject
issued
by
the
Federal
Railroad Administration
(49
CFR
Part 219
"Con-
trol
of
Alcohol and
Drug
Use
in Railroad
Oper-
ation")
and other pertinent legal authorities,
copies
of
which
are
available
for
review upon
request
Concurrently,
Santa
Fe
provides
positive
con-
ditions encouraging employees to
seek relief
from
a
need to
use
or
abuse these
substances
by
utiliz-
ing
the
Employee Assistance Program
(EAP).
2
0
GENERAL POLICY
This
policy
supplements,
but
does
not
replace,
disciplinary
rules
and procedures currently in
force relating to violations involving use of
alcohol
and drugs
2
1
Toxicologies]
Testing
Toxicology tests
for the
presence
of
drugs
are
conducted
when conditions
exist
as
outlined
by
statutes
or
regulations
and
applicable
Santa
Fe
policy
An
employee whose sample
tests
posi-
tive
is
conclusively
presumed
to
be
incapable
of
safely
or
properly
performing
the
duties
of
the
position
for
which employed
and is
subject
to
the
conditions
outlined
in this
policy
2
2
Drugs
The
word
"drugs"
refers to controlled
sub-
stances which can influence or impair one's
judgment,
reaction
and
behavior
Controlled
sub-
stances include
illicit
drugs and certain drugs
which
may
only
be
distributed
by
a
medical
prac-
titioner's prescription
or
authorization,
such
as
marijuana,
narcotics,
stimulants,
depressants
and
hallucinogens
3 0 VOLUNTARY REFERRAL POLICY
This provision applies to employees who
volun-
tarily
seek
the
aid
of
the
EAP
3
1
Eligibility
An employee
is
eligible
for
the
provisions
of
Voluntary Referral
whether
self-referred
(seek-
ing assistance on one's own) or referred by
another employee
or
by
the
employee's collec-
tive
bargaining representative
An
employee
is
not eligible
for
the
provisions
of Voluntary Referral
if,
prior
to
seeking as-
sistance,
the
employee has been charged with
conduct which
is
in violation
of
Santa
Fe
rules
regarding
the use
of
alcohol and
drugs,
or if
the
employee
is
in violation
of
such Santa
Fe
rules
at the time
of
referral
3.2 Leave
of
Absence
Leave of absence
for
medical reasons
without
pay
will
be
granted
under
provisions
of
Voluntary
Referral
when recommended by the
Medical Director
-
System or the employee's
physician,
to allow
treatment
in
a
rehabilitation
program
outlined
by
an
EAP
counselor
The
dur-
ation
of
said
leave
of
absence
will
be
at
least
45
days,
if
necessary,
to
complete treatment
Such
leave
of
absence
may
be
continued
until
determined
by
the
Medical
Director
-
System that
it
is
appropriate
to return
the
employee
to
work.
3
3
Confidentiality
An
eligible employee
who seeks
assistance
2
3
APPENDIX
E 60
under
this Voluntary Referral provision
will
be
treated
on
a
strictly confidential
basis.
4
0
CO-WORKER REPORT POLICY
These
provisions
control
when employees
are
reported
by
their
co-workers to
be
in
violation
of
rules prohibiting
the use
of
alcohol and
drugs
4
1
Eligibility
Exclusively
for
purposes
of
this
Co-Worker
Report
Policy,
the
terms
"employee"
and "Co-
Worker"
exclude
(a)
exempt
personnel
who do
not perform
service
in
a
craft
or
class
of
em-
ployees
of
this
Carrier
and
whose
responsibilities
are
primarily
and
essentially
supervisory,
man-
agerial
or
professional in
nature
and
(b)
Santa
Fe
special
agents
For
any
given
employee,
the
provisions
of
this
Co-Worker Report Policy may be invoked
only
once.
Also,
these
provisions
are
only ap-
plicable
when
that
employee's violation
of
Santa
Fe
rules on
alcohol
and
drug
use
is
brought
to
the
attention
of
a
Santa Fe
official
exclusively
through
the
report
of
a
co-worker
Eligibility
for
the
benefit
of
the
Co-Worker
Report
Policy will
continue
only
so long
as
the
employee
conforms to
all
requirements outlined
in
the
procedures
below.
4
2
Co-Worker Report Policy Procedure
In
order
to
report
a
fellow
employee for
violation
of
Santa
Fe
rules on
alcohol and
drug
use,
a
co-worker
reports
the
suspected
violator
to
a
Santa
Fe
official.
When
such
a
report
is
received,
a
compa-
ny
official
will
observe
the
alleged
violator
to
de-
termine whether
a
violation
has
occurred
If,
in
the
official's
judgment,
an
employee
is
in
viola-
tion,
the
employee
will
be
suspended
from
serv-
ice
immediately pending formal investigation.
4
3
Excuse
of
Discipline
An
employee eligible
for
treatment
under
the
provisions
of
this
Co-Worker Report
Policy
may avoid discipline based on the co-worker
report
and
maintain an
employment
relationship
with Santa
Fe
provided
the
employee
fulfills
all
conditions outlined
below:
4
3
1
A
waiver
will
be
included with
the
notice
served
for
formal
investigation
ac-
cording to current practices and agree-
ments A
reported
employee
who signs this
waiver
will*
1)
waive the investigation,
2)
agree
to undergo
an evaluation by the
EAP
counselor,
and
3)
if
found
to
be
de-
pendent on
a
prohibited
substance,
agree
to satisfactorily complete a program of
treatment outlined by
the
counselor
4
3 2
If
the
employee
elects to
waive
the
investigation
and
be
evaluated
for
alcohol
or
drug
abuse,
the
waiver
form
(example
on
page
10)
must
be
completed
and
signed
1) by
the
employee,
2)
where
applicable,
witnessed
by
an
appropriate
union
repre-
sentative,
and
3)
delivered to
the
company
official who issued
the
notice
of investiga-
tion within
five
(5)
calandar
days
from
the
date the
notice
of
investigation
was
received
by
the
employee.
4
33 The
employee must contact
an
EAP
counselor to arrange
for
the evaluation
within
three
(3)
calendar
days
from
the date
the
signed waiver
is
delivered
to
the
ap-
propriate
company
official
as
specified in
Section
4
3.2.
4.3.4 The EAP
counselor
will
schedule
the
necessary interviews
and
complete
the
evaluation
not later
than ten
00)
calendar
days
from
the date
of
contact
by
the
em-
ployee
4
3.5
An
employee whose
evaluation
in-
dicates no dependency on
the use
of alco-
hol or
drugs wflj
be returned
to
service
within
5
days
of
completion
of
the
evalua-
tion,
consistent
with
the
recommendation
of
the
Medical
Director
-
System
and
stan-
4
5
61
APPENDIX
E
dard Santa
Fe
practices,
and may
be
sub-
ject
to conditions outlined in Sections
6.0
and
6.Z
4
36
During
the
out-of-service
period
or
following
return to
service
outlined in
Sec-
tion 4 3
5,
the
employee may
be
required
to
participate
in
a
program
of
education
and
training
concerning
the
effects
of
alcohol
and
drugs
on occupational/transportation
safety, as the EAP counselor deems
necessary'
4
37
An
employee
who
fells
to
continue
treatment may be withheld from service
and
placed
on.
a
medical
leave
of
absence
by
the
Medical
Director
-
System
The
em-
ployee's
failure
may
also
be
reported
by
the
counselor
to
Santa Fe
officials
4
38
An
employee whose
evaluation
in-
dicates
dependence on
the use
of
alcohol
or
drugs
must
satisfactorily
complete
a
pro-
gram
of
primary
and
follow-up
treatment
as
outlined
by
the
EAP
counselor
An em-
ployee
will
be
given an unpaid
leave
of
ab-
sence
of
up
to
45
days,
if
necessary,
for
purposes
of
meeting
treatment
needs
Upon
completion
of
the
primary
treatment,
the
employee will be returned to service
promptly,
consistent
with
the
recommen-
dation
of
the
Medical Director
-
System
and standard Santa
Fe
practices
Follow-
up
treatment
deemed necessary
by
the
EAP
counselor
extends
for
a
period
of
two
(2)
years
from
the date
of
the
report.
4.4 Leave
of
Absence
A
leave
of
absence without
pay
for
medi-
cal
reasons
will
be
granted an
employee eligible
under Co-Worker Report
Policy
provisions
when
such
leave
is
recommended
by
the
Medical
Direc-
tor
-
System
for
treatment
Such
leave
of absence
may
be
continued
.until
determined
by
the
Medi-
cal Director
-
System
that
it
is
appropriate to
return
the
employee
tq
work
The
duration
of said
leave
of
absence will.be
at
least
45
days,
if
neces-
sary,
to
complete,
treatment
4.5 Co-Worker
as
Witness
In no
case
will
a
co-worker
who
reports
an
employee's violation
of
Santa
Fe
rules
concern-
ing
alcohol and
drug
use
be
required
to
appear
or
otherwise participate
in
a
formal
investigation
conducted
in connection with
that
reported
em-
ployee's alleged
alcohol and
drug
rule
violation.
4.6
Intent
Nothing
in this
Co-Worker Report
Policy
is
intended
or
shall
be
construed to
create
or
form
the
basis
of
a
contract
or
covenant
of employment
between Santa
Fe
and
any
employee
or
group
of
employees
5 0 REINSTATEMENT
An
employee
who
is
dismissed
for
violating
ex-
isting
Company
rules covering
alcohol and
drug
use
will
not
be
considered
for
reinstatement
to
service
until
after
an evaluation
has
determined
medical
fitness
of
the
individual,
and
a
favorable
recommendation
is
received
from
the
EAP
coun-
selor
through
the
Medical Director
-
System
6
0
MEDICAL EXAMINATIONS
All
return-to-service,
periodic
and
other
em-
ployee
medical
examinations provided
for
by
the
Medical Director-System include
a
urine
drug
screen analysis
6.1 Urine
Tests
Positive
For
Drugs
Individuals
examined
under
provisions
of
Section
6.0
whose urine
tests
positive
for
a
sub-
stance,
the use
of
which
is
prohibited
by
Federal
Railroad Administration regulations, will be
placed on
medical
leave
of absence Subsequent-
ly,
these
employees
will
be
instructed in writing
to
rid
their system
of
drugs
and
within
60
days
must:
1)
undergo
evaluation
by
the
EAP counselor,
2)
abide
by
the
counselor's
recommendations,
3)
provide
a
negative urine
specimen
An
employee
in
a
treatment program
ex-
6 7

APPENDIX
E 62
tending
beyond
the
60
day
period
must provide
a
negative urine
specimen
within
five
(5)
days
of
discbarge
from
the
program Failure
to
abide
by
these
conditions
will
subject
the
employee
to
dismissal
for
disobeying instructions.
A
decision
by
the
Medical
Director
-
Sys-
tem
to
withhold
an
employee from
service
un-
der
Section
6
of
this
policy is
not
and shall
not
be
considered discipline.
6
2
Follow-Up Testing
An
employee
who provides
a
negative urine
specimen and
has
been permitted
to
return to
service
is
subject,
for
a
period
of
two
(2)
years,
to
urine
testing
as
determined by
the
Medical
Director
-
System
If
such
further
testing
is
posi-
tive,
the
employee
will
be
placed on
medical
leave
of
absence
Such an
employee
will
be
subject
to
the
same
conditions
set
forth
in
Section 61
RANDOM DRUG TESTING PROGRAM
In
order
to
comply
with regulations issued
by
the
Federal
Railroad
Administration,
employees
who
perform service
covered
by
the
provisions
of
the
Hours of Service Act are required to
undergo
random urine
testing
for use
of
certain
prohibited
or
controlled drugs Selection
of
in-
dividuals who
must provide urine
samples
is
en-
tirely
random and computer generated
Employees selected
for
such testing
will
be
asked
either
immediately
after
reporting
for
duty
or
before
going
off-duty
to
accompany
a
super-
visor
to
a
facility
where
urine
samples
will
be
collected by approved
personnel.
Employees
who,
upon
being notified
of
their
selection
for
testing,
refuse
to
participate
will
be
disqualified
from covered
service
for
a
minimum
period
of
nine
(9)
months
Upon
the
expiration
of
this
dis-
qualifying
period,
said employees
must provide
negative urine
specimens
before
being
permit-
ted
to return to
covered service
7.1 Handling
of
Test
Results
Employees who have provided urine
samples
under
requirements
of
this
Random
Drug
Testing Program
are advised
in
writing
of
the
results
of
their respective
tests Individuals
whose
specimens
test
positive
will
be
provided
with
a
copy of the
relevant laboratory
reports. These em-
ployees
will
be instructed to contact the
Medical
Director - System within five (S) working days
of
receipt
of
the
written notifications to
discuss,
confidentially,
the results of their tests
Failure
to
contact
the
Medical
Director
-
System
as
outlined
above
and
provide
documen-
tation to
his
satisfaction
will
result
in
medical
dis-
qualification
of
the
employee
7.2 Medical Disqualification
Employees
who
are
medically disqualified
as
a
result
of
positive urine
samples
will
remain
in said status
until they
have
fulfilled
the
condi-
tions
set
forth
in
Section
6.1.
7 3 Follow-Up Testing
Employees who provide negative urine
samples and
are
permitted
to return to
service
will
be
subject
to
the
same
conditions
outlined
in Section
6.2
8 0 ADMINISTRATION
Any
questions
regarding
this
policy
should be
referred to
the
Vice-President
Human Resources
8
9
63
APPENDIX
E
EXAMPLE
(Official to
Whom Sent)
Employee Assistance
Program Counselors
(address)
WAIVER
i,
by affixing
my
signature
below,
waive
my
rights
to
for-
mal
investigation,
scheduled on
,
to develop facts and place
my
responsibility,
if
any,
in
connection with
my
being relieved from duty
in
suspected violation
of
Rule
G,
General Code
of
Operating Rules while performing service
as a
on
I understand that
discipline,
if
any,
to be
imposed
_
a result of the
incident
to
be investigated
will
be
excused,
provided
I contact the
EAP
counselor
with-
in three
(3)
calendar days
from
the date this waiver is
executed,
and thereafter enter into the program
of treat-
ment prescribed
I further understand and agree that any failure
on
my
part to
complete
the
prescribed program
of
treat-
ment
will result in
my
being placed on medical leave
of absence with release to return to service to
come
only from
the
Medical Director
-
System
(Signature)
Eastern Region:
Terry L. Cordray
Program Manager
4515 Kansas Avenue
Kansas City, KS 66106
(913) 551-4465
Ext. 4465
Western Region:
Bruce J. Rehberg
1441 W Airport Freeway
Euless, TX 76040
(817) 868-3196
Ext 3196
James L Harrell
740 E. Carnegie Dr
San Bernardino, CA 92408-3571
(714) 386-4151
Ext. 4151
Witness.
(SSA
Dumber)
(Signature)
(Union
Title
of
Witness)
Receipt Acknowledged
(Signature)
(Tuie)
(Due)
10
11
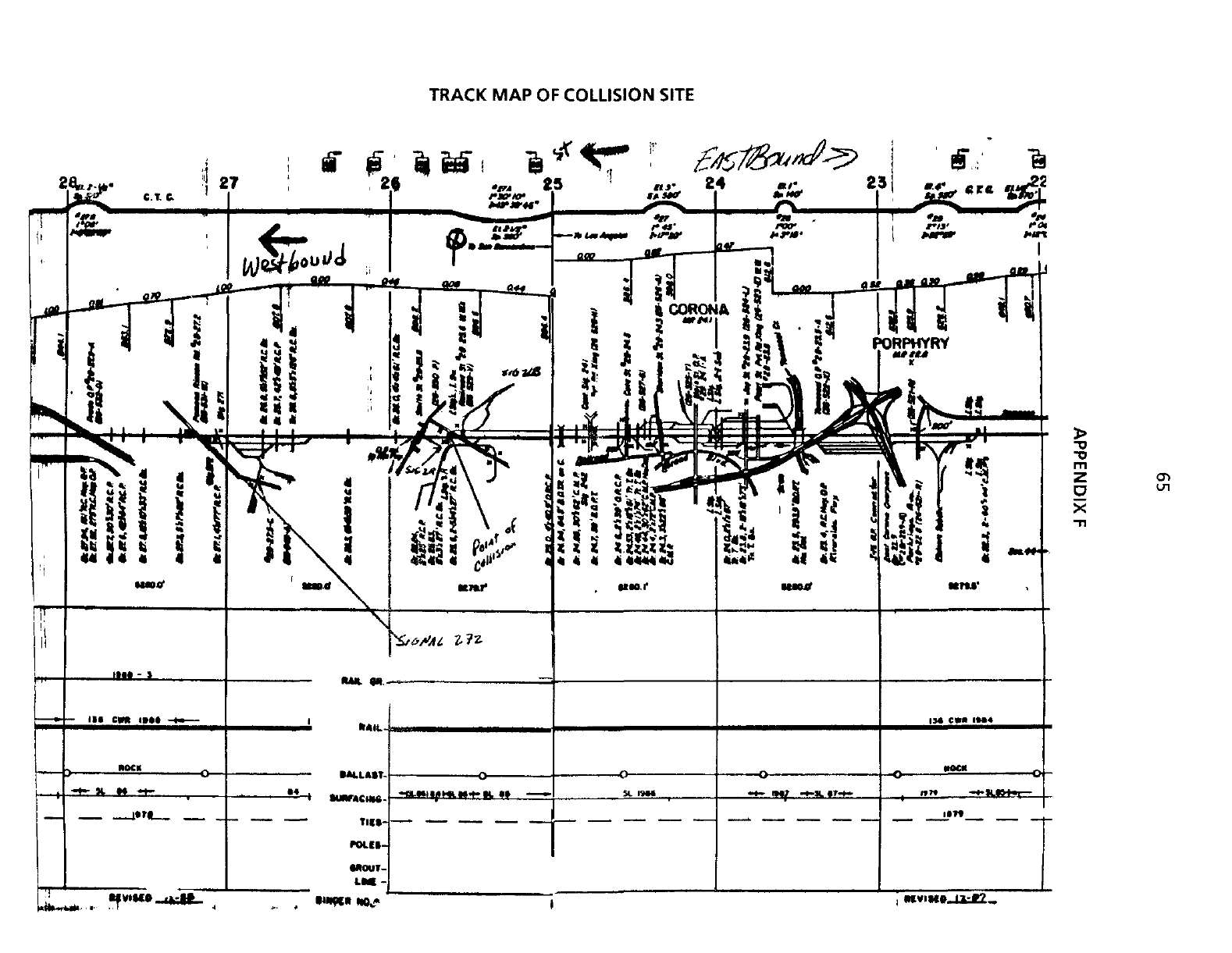
TRACK
MAP OF
COLLISION SITE
24 */- 23
?a\
5
PORPHYRY
MVISW.J&J2..
