
CollisionofMetrolinkTrain111With
UnionPacificTrainLOF65‐12
Chatsworth,California
September12,2008
Accident Report
NTSB/RAR-10/01
National Transportation Safety Board
PB2010-916301
National
Transportation
Safety Board
NTSB/RAR-10/01
PB2010-916301
Notation 8175
Adopted January 21, 2010
Railroad Accident Report
Collision of Metrolink Train 111 With
Union Pacific Train LOF65-12
Chatsworth, California
September 12, 2008
National
Transportation
Safety Board
490 L’Enfant Plaza, S.W.
Washington, D.C. 20594

National Transportation Safety Board. 2010. Collision of Metrolink Train 111 With Union Pacific Train
LOF65–12, Chatsworth, California, September 12, 2008. Railroad Accident Report NTSB/RAR-10/01.
Washington, DC.
Abstract: About 4:22 p.m., Pacific daylight time, on Friday, September 12, 2008, westbound Southern
California Regional Rail Authority Metrolink train 111, consisting of one locomotive and three passenger cars,
collided head-on with eastbound Union Pacific Railroad (UP) freight train LOF65–12 near Chatsworth,
California. The Metrolink train derailed its locomotive and lead passenger car; the UP train derailed its 2
locomotives and 10 of its 17 cars. The force of the collision caused the locomotive of train 111 to telescope into
the lead passenger coach by about 52 feet. The accident resulted in 25 fatalities, including the engineer of train
111. Emergency response agencies reported transporting 102 injured passengers to local hospitals. Damages
were estimated to be in excess of $12 million.
The National Transportation Safety Board (NTSB) is an independent federal agency dedicated to promoting aviation, railroad,
highway, marine, pipeline, and hazardous materials safety. Established in 1967, the agency is mandated by Congress through the
Independent Safety Board Act of 1974 to investigate transportation accidents, determine the probable causes of the accidents, issue
safety recommendations, study transportation safety issues, and evaluate the safety effectiveness of government agencies involved in
transportation. The NTSB makes public its actions and decisions through accident reports, safety studies, special investigation reports,
safety recommendations, and statistical reviews.
Recent publications are available in their entirety on the Internet at <http://www.ntsb.gov>. Other information about available
publications also may be obtained from the website or by contacting:
National Transportation Safety Board
Records Management Division, CIO-40
490 L’Enfant Plaza, SW
Washington, DC 20594
(800) 877-6799 or (202) 314-6551
NTSB publications may be purchased, by individual copy or by subscription, from the National Technical Information Service. To
purchase this publication, order report number PB2010-916301 from:
National Technical Information Service
5285 Port Royal Road
Springfield, Virginia 22161
(800) 553-6847 or (703) 605-6000
The Independent Safety Board Act, as codified at 49 U.S.C. Section 1154(b), precludes the admission into evidence or use of NTSB
reports related to an incident or accident in a civil action for damages resulting from a matter mentioned in the report.

NTSB Railroad Accident Report
National Transportation Safety Board iii
Contents
Contents ........................................................................................................................................ iii
Figures .............................................................................................................................................v
Acronyms and Abbreviations ..................................................................................................... vi
Executive Summary .................................................................................................................... vii
Factual Information .......................................................................................................................1
Accident Synopsis ............................................................................................................................1
Accident Narrative ...........................................................................................................................1
Emergency Response .......................................................................................................................8
Command, Organization, and Resources ..................................................................................9
Extrication Operations ............................................................................................................10
Injuries ...........................................................................................................................................11
Damage ..........................................................................................................................................11
Personnel Information ....................................................................................................................12
Metrolink Train 111 ................................................................................................................12
Union Pacific Leesdale Local .................................................................................................13
Person A ..................................................................................................................................14
Train and Mechanical Information ................................................................................................15
Metrolink Train 111 ................................................................................................................15
Leesdale Local ........................................................................................................................18
Wreckage .......................................................................................................................................19
Metrolink Train 111 ................................................................................................................19
UP Leesdale Local ..................................................................................................................22
Topanga Switch ......................................................................................................................22
Meteorological Information ...........................................................................................................22
Track Information ..........................................................................................................................22
Signal Information .........................................................................................................................24
General ....................................................................................................................................24
Review of Recorded Signal Data ............................................................................................25
Operations Information ..................................................................................................................25
General ....................................................................................................................................25
Operating Rules and Efficiency Testing .................................................................................27
Medical and Toxicological Information ........................................................................................27
Metrolink Engineer’s Use of a Wireless Device ............................................................................28
Pattern of Wireless Device Use ..............................................................................................29
Content of Text Messages ......................................................................................................34
Leesdale Local Conductor’s Use of a Wireless Device .................................................................35
Tests and Research .........................................................................................................................36
Sight-Distance Tests of Trains ................................................................................................36
Sight-Distance Tests of Signals ..............................................................................................37

NTSB Railroad Accident Report
National Transportation Safety Board iv
Testing of Signal System ........................................................................................................39
Testing of Communications System .......................................................................................40
Inspection and Testing of Track .............................................................................................41
Other Information ..........................................................................................................................41
Postaccident Actions by SCRRA ............................................................................................41
Federal Rules Regarding Wireless Devices ............................................................................43
FRA Emergency Order 20 (1996) ..........................................................................................44
Analysis .........................................................................................................................................46
Exclusions ......................................................................................................................................46
The Accident ..................................................................................................................................48
Emergency Response .....................................................................................................................49
Signals and Train Control ..............................................................................................................50
Signal Aspect at CP Topanga .................................................................................................50
Stacking of Routes ..................................................................................................................51
Perceptions of Signal Aspects ................................................................................................51
Performance of Train 111 Engineer ...............................................................................................53
Train 111 Engineer’s Use of Wireless Device ...............................................................................55
Leesdale Local Conductor’s Use of Wireless Device ....................................................................55
Unauthorized Persons in Locomotive Cab ....................................................................................56
Efficiency Testing and Management Oversight ............................................................................56
In-Cab Audio and Image Recording Devices ................................................................................58
Metrolink Passenger Survivability .................................................................................................62
Positive Train Control ....................................................................................................................63
Conclusions ...................................................................................................................................65
Findings..........................................................................................................................................65
Probable Cause...............................................................................................................................66
Recommendations ........................................................................................................................67
New Recommendations .................................................................................................................67
Previously Issued Recommendation Reclassified in This Report .................................................67
Appendix A: Investigation ..........................................................................................................72
Appendix B: Recommendation History on Employee Performance Monitoring ..................73

NTSB Railroad Accident Report
National Transportation Safety Board v
Figures
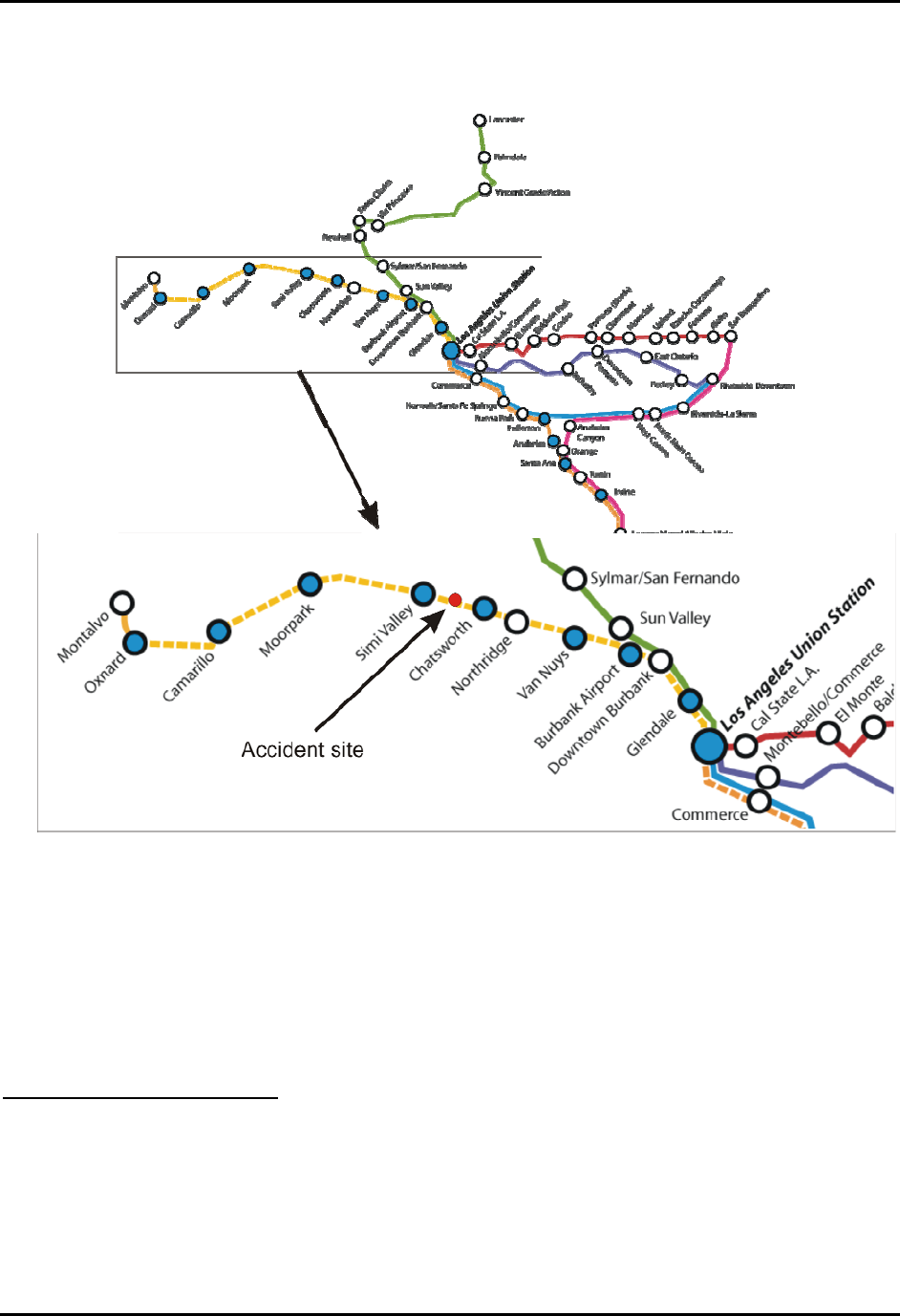
Figure 1. The accident occurred on Metrolink's Ventura Subdivision, about 33 miles
west of Los Angeles. ........................................................................................................................2
Figure 2. Accident site. ......................................................................................................5
Figure 3. CP Topanga as viewed from the cab of a locomotive positioned at Chatsworth
station. Upper arrow indicates approximate location of the CP Topanga signal, which is about
5,288 feet away. ...............................................................................................................................6
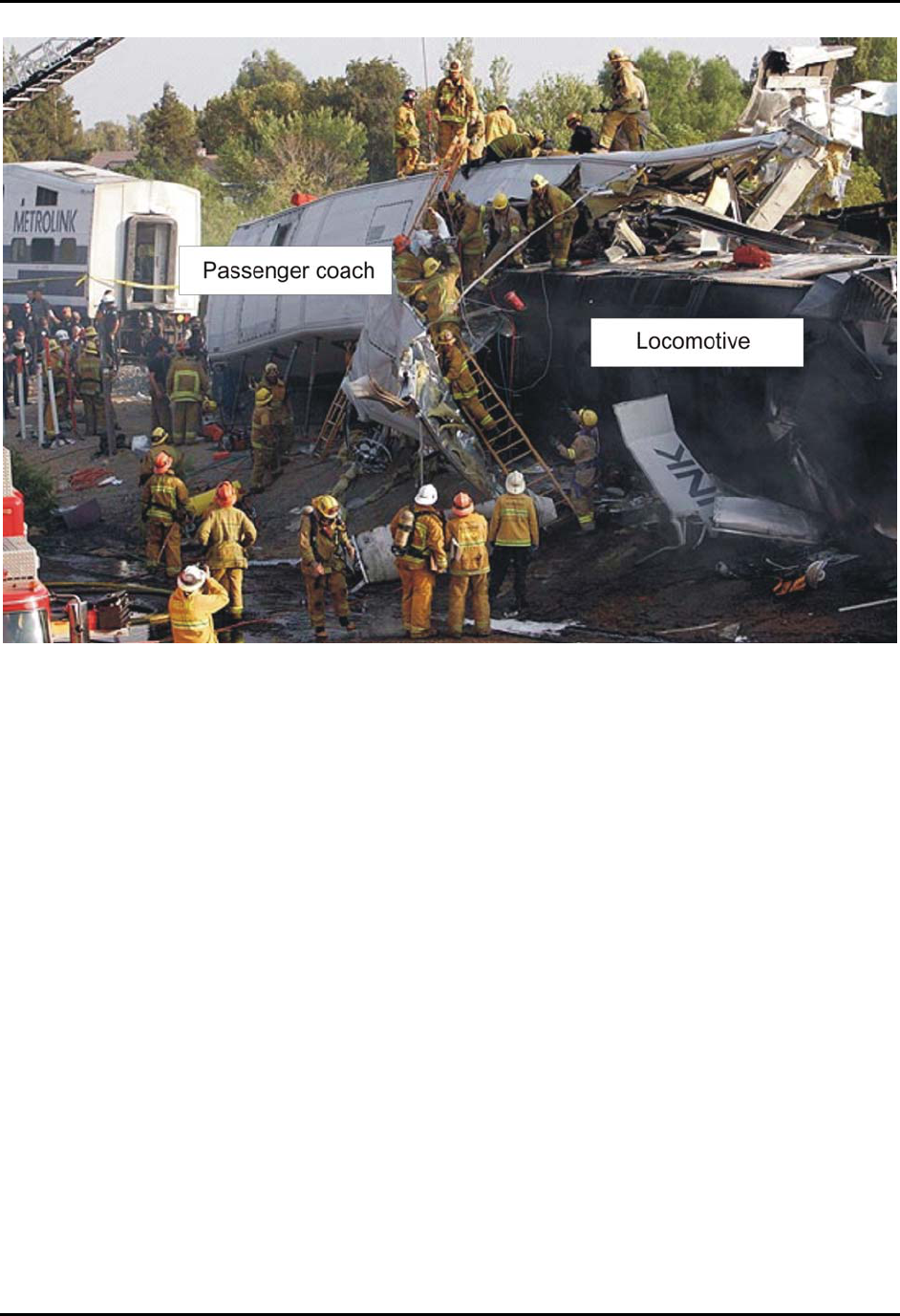
Figure 4. Overview of accident scene looking south. . .......................................................8
Figure 5. Bombardier BiLevel passenger coach of the type involved in this accident. . ..15
Figure 6. The force of the collision drove the Metrolink locomotive about 52 feet into the
passenger space of the first coach behind the locomotive. . ..........................................................20
Figure 7. CP Topanga switch looking east, in the direction the Leesdale Local was
traveling. Circles highlight damage to switch points and components consistent with the switch
having been run through in a trailing point movement by the Metrolink train traveling in the
opposite direction. .........................................................................................................................23
Figure 8. Westbound signal at CP Topanga displaying a red aspect (indicating stop.). ..26
Figure 9. LG wireless device Model VX10000 similar to the device used by the
Metrolink engineer on the day of the accident. (Internet photograph) ..........................................29
Figure 10. Text messages sent and received by the Metrolink engineer on day of the
accident and on previous 7 days. (Engineer did not work Saturday or Sunday.) ..........................32
Figure 11. Telephone calls sent and received by Metrolink engineer on day of accident
and on previous 7 days. ..................................................................................................................33
Figure 12. View from the head end of a simulated Leesdale Local during train sight-
distance testing. At a closing speed in excess of 80 mph, the trains would be only seconds from
impact as the Metrolink train becomes visible around the curve. . ................................................37

NTSB Railroad Accident Report
National Transportation Safety Board vi
Acronyms and Abbreviations
BMI body mass index
CFR Code of Federal Regulations
Connex Connex Railroad, LLC
CP control point
FRA Federal Railroad Administration
GPS global positioning system
HIV human immunodeficiency virus
NTSB National Transportation Safety Board
OSA obstructive sleep apnea
SCRRA Southern California Regional Rail Authority
UP Union Pacific Railroad

NTSB Railroad Accident Report
National Transportation Safety Board vii
Executive Summary
About 4:22 p.m., Pacific daylight time, on Friday, September 12, 2008, westbound
Southern California Regional Rail Authority Metrolink train 111, consisting of one locomotive
and three passenger cars, collided head-on with eastbound Union Pacific Railroad freight train
LOF65–12 near Chatsworth, California. The Metrolink train derailed its locomotive and lead
passenger car; the UP train derailed its 2 locomotives and 10 of its 17 cars. The force of the
collision caused the locomotive of train 111 to telescope into the lead passenger coach by about
52 feet. The accident resulted in 25 fatalities, including the engineer of train 111. Emergency
response agencies reported transporting 102 injured passengers to local hospitals. Damages were
estimated to be in excess of $12 million.
The National Transportation Safety Board determines that the probable cause of the
September 12, 2008, collision of a Metrolink commuter train and a Union Pacific freight train
was the failure of the Metrolink engineer to observe and appropriately respond to the red signal
aspect at Control Point Topanga because he was engaged in prohibited use of a wireless device,
specifically text messaging, that distracted him from his duties. Contributing to the accident was
the lack of a positive train control system that would have stopped the Metrolink train short of
the red signal and thus prevented the collision.
The safety issues identified during this accident investigation are as follows:
• Inadequate capability, because of the privacy offered by a locomotive operating
compartment, for management to monitor crewmember adherence to operating rules
such as those regarding the use of wireless devices or the presence of unauthorized
persons in the operating compartment.
• Lack of a positive train control system on the Metrolink rail system.
As a result of its investigation of this accident, the National Transportation Safety Board
makes recommendations to the Federal Railroad Administration.

(This page intentionally left blank)

NTSB Railroad Accident Report
National Transportation Safety Board 1
Factual Information
Accident Synopsis
About 4:22 p.m., Pacific daylight time,
1
on Friday, September 12, 2008, westbound
Southern California Regional Rail Authority (SCRRA) Metrolink train 111, consisting of one
locomotive and three passenger cars, collided head-on with eastbound Union Pacific Railroad
(UP) freight train LOF65–12 near Chatsworth, California. The Metrolink train derailed its
locomotive and lead passenger car; the UP train derailed its 2 locomotives and 10 of its 17 cars.
The force of the collision caused the locomotive of train 111 to telescope into the lead passenger
coach by about 52 feet. The accident resulted in 25 fatalities, including the engineer of train 111.
Emergency response agencies reported transporting 102 injured passengers to local hospitals.
Damages were estimated to be in excess of $12 million.
Accident Narrative
At 5:54 a.m. on the morning of the accident, the two-member crew (conductor and
engineer) who were aboard Metrolink train 111 at the time of the accident reported for duty at
the Metrolink crew base in Montalvo, California. Once on duty, the crew participated in a job
briefing where they discussed track warrants and bulletins from the various territories over which
they would be operating that day. The crew departed the yard eastbound
2
about 6:45 a.m. aboard
train 106. The train made 10 station stops before arriving at Los Angeles Union Station at 8:25
a.m. (See figure 1.) At 8:32 a.m. the crewmembers took the train a few miles west to Metrolink’s
central maintenance facility, where they went off duty at 9:26 a.m. The conductor said he then
went upstairs to the “quiet” room provided for employees and that the engineer, as was his usual
practice during the mid-day relief,
3
drove home.
At 11:30 a.m. the three-member crew (engineer, conductor, and brakeman) of UP freight
train LOF65–12 (hereinafter referred to as the Leesdale Local) reported for duty in Gemco,
California. The Leesdale Local departed Gemco westbound at 12:30 p.m. with orders to service
local industries along the route.
The Metrolink train crew returned to duty at the central maintenance facility at 2:00 p.m.
The conductor said the engineer spoke of having gotten a 2-hour nap during the mid-day break.
The crew participated in a job briefing and was issued new track bulletins. They then traveled to
the yard, boarded the equipment scheduled for train 111—which consisted of one locomotive,
1
Unless otherwise noted, all times in this report are Pacific daylight time.
2
Unless otherwise noted, directions referred to in this report are railroad timetable directions, which often differ
from compass direction.
3
The Metrolink train crew worked split shifts. They operated trains during the morning and afternoon rush
periods and were off during the middle of the day.
NTSB Railroad Accident Report
two regular passenger cars, and one passenger coach/cab control car
4
—and departed at 3:03 p.m.
in non-revenue service from the maintenance facility to Union Station, arriving at 3:12:03 p.m.
Figure 1. The accident occurred on Metrolink's Ventura Subdivision, about 33 miles west of Los
Angeles.
Verizon Wireless records of calls and text messages to and from the engineer’s personal
cell phone/wireless device showed that while the engineer was en route from the maintenance
facility to Union Station he received a text message from an individual who will be referred to in
this report as “Person A.”
5
This was the first of seven text messages Person A transmitted to the
engineer from the time train 111 departed the maintenance facility until the accident.
4
The trains operated by the crew on the day of the accident were commuter trains configured in a “push-pull”
arrangement that allows the train to operate in either direction without being turned. In the “pull” mode, the engineer
operates from the locomotive at the head end of the train. In the “push” mode, the locomotive is at the rear of the
train and the engineer occupies the operating compartment of a cab control car (a specially configured passenger
coach) that, in the push mode, is at the head end of the train. At the time of this accident, the train was operating in
the pull mode, and the engineer was in the locomotive at the head end.
5
As will be discussed later in this report, the engineer had, earlier in the day, exchanged a number of text
messages with the individual identified as Person A.
National Transportation Safety Board 2
NTSB Railroad Accident Report
National Transportation Safety Board 3
While train 111 was at Union Station and before it began its westbound trip, the engineer
received the second text message from Person A. The records indicated that the engineer
responded with two text messages to Person A, the first sent at 3:23:59 p.m. and the next at
3:30:49 p.m.
6
These were the first of six text messages the engineer would transmit to Person A
that afternoon. At 3:21:42 p.m. and again at 3:26:11 p.m., the engineer made two cell phone
calls, each lasting 75 seconds, to two different phone numbers (neither of them belonging to
Person A). These were the only voice calls the engineer made while he was on duty on the
afternoon of the accident.
Meanwhile, the Leesdale Local had completed its westbound work assignments at
Oxnard, California, and, at 3:13 p.m., had begun its eastbound return trip to Gemco, which is
near the Metrolink Van Nuys station. The Leesdale Local departed Oxnard with two locomotive
units pulling 17 cars. For this return trip, the engineer and the conductor were in the lead
locomotive while the brakeman rode the trailing unit.
Train 111 departed Los Angeles Union Station westbound on schedule at 3:34:54 p.m.
7
en route to Moorpark, California. The engineer occupied the locomotive at the head end of the
train, and the conductor was in the last passenger car. The train would be operating on double
main line track until reaching Control Point (CP)
8
Raymer (located between the Van Nuys and
Northridge stations), where the main line became single track. About 1 minute into the trip, the
engineer received the third text message from Person A.
Train 111’s first two scheduled stops were Glendale and Downtown Burbank. As the
train pulled away from the Downtown Burbank station, at 3:51:08, the Verizon network logged
the transmission of the engineer’s third text message to Person A. The engineer received the
fourth text message from Person A while en route between the Burbank–Bob Hope Airport and
Van Nuys stations, and the fifth while en route between the Van Nuys and Northridge stations.
At this time, eastbound Amtrak train 784 was operating on the single track portion of the
mainline and on the same track as train 111. The Metrolink dispatcher
9
had aligned switches to
route the Amtrak train onto the adjacent main line track at CP Raymer to allow the two trains to
pass. Because the switch at CP Raymer was aligned for the eastbound Amtrak train’s movement
and against any westbound movement, the signal at the control point showed a red aspect, a stop
indication, for train 111. Metrolink’s operations center radio recordings captured the train 111
6
In this report, all times associated with the sending or receiving of calls and text messages are from Verizon
records. In these records, the “sent” and “received” times are based on a GPS time reference and reflect the time the
Verizon Wireless network equipment either receives or delivers a message. Thus, the reported “sent” time of a
message does not necessarily correlate to the time the sender pressed the “send” button on the wireless device.
Because the network must query the receiving device to make sure it is available before transmitting a message, the
“received” time is more likely to reflect the actual time the message arrives on the recipient’s device.
7
In this report, all times associated with signal, switch, and locomotive events are based on signal log and
locomotive event recorder data synchronized to a GPS reference time. This synchronization correlates train position,
data recorder, signal, and cell phone send/receive times to a common “master clock” that reflects actual GPS time.
8
A control point is a signal or a siding or crossover switch that is under the control of the dispatcher and that
the dispatcher uses to manage train movements over the territory.
9
The dispatcher referred to in this report was responsible for all train movements over the territory extending
from Glendale to Moorpark.
NTSB Railroad Accident Report
National Transportation Safety Board 4
engineer calling this signal (“all red Raymer”).
10
After servicing the Van Nuys station, train 111
stopped short of the CP Raymer signal at 4:06:54 to wait for the Amtrak train to move to the
other track and for the signal to clear for continued westbound movement. The wait lasted about
3 minutes, during which Verizon records show that the train 111 engineer transmitted the fourth
and fifth of his six text messages to Person A. At the end of the stop, the engineer was recorded
calling “back in green” (clear) at Raymer.
About 2 minutes after train 111 departed CP Raymer, at 4:11 p.m., the eastbound
Leesdale Local entered the single track mainline (the same track as train 111) at CP Davis
traveling at a recorded speed of 46.6 mph. The dispatcher had aligned the switches so that the
eastbound local would enter the 11,300-foot-long controlled siding at CP Topanga, just west of
the Chatsworth station. (See figure 2.) The signal circuitry was designed such that, with this
switch aligned for the siding, the westbound signal at CP Topanga could not display any aspect
other than red (stop indication) for westbound trains entering the block of track
11
governed by
that signal. This indication required that train 111 stop short of CP Topanga until the Leesdale
Local was safely in the siding. Once the train was in the siding, the switch would be realigned for
westbound movement on the main line, the signal would be cleared, and train 111 could
proceed.
12
Signal data logs showed that the switch at CP Topanga was reversed (aligned for the
siding) at 4:07:37 p.m.
Train 111 arrived at Northridge station at 4:14:10 p.m. and departed 40 seconds later.
Normal travel time between the Northridge and Chatsworth stations is about 6 minutes. The
conductor of train 111 stated that after the train departed Northridge, he began walking through
the train. Dispatching center recordings showed that, after departing Raymer, the train 111
engineer called the next three intermediate signals as “green.” The next signal the train
encountered was the signal at CP Bernson (milepost 446.8), for which Metrolink’s operations
center recorded the train 111 engineer calling a flashing yellow aspect (advance approach).
Under an advance approach signal indication, trains are to “proceed prepared to stop at second
signal.” In this case, the second signal was the signal at CP Topanga, where train 111 was to stop
and wait for the Leesdale Local to clear the main line. The train passed the CP Bernson signal at
4:17:45 p.m. at a recorded speed of 68 mph. Under Metrolink rules, the conductor of a train must
repeat back over the radio any restrictive signal (an indication other than clear) called out by the
engineer. Train 111’s conductor was not recorded repeating back the flashing yellow signal the
engineer called at CP Bernson. The conductor said he did not recall hearing the engineer call this
signal. A few seconds after train 111’s engineer was recorded calling out the flashing yellow
aspect at CP Bernson, the engineer of the Leesdale Local was recorded calling out a “green”
aspect at CP Davis. Signal data logs showed that this signal had cleared at 4:10:59 p.m.
10
Metrolink operating rules require that engineers announce over the radio the aspects or indications of all
wayside signals the train encounters. For an announcement of any signal more restrictive than green (clear), the
conductor must repeat back the announcement over the radio.
11
A block is a length of track of defined limits, the movement over which is governed by wayside signal
indications
12
As will be discussed later in this report, the commands by the dispatcher to effect these actions had already
been “stacked,” or entered into the dispatching system at the Metrolink Operations Center.
NTSB Railroad Accident Report
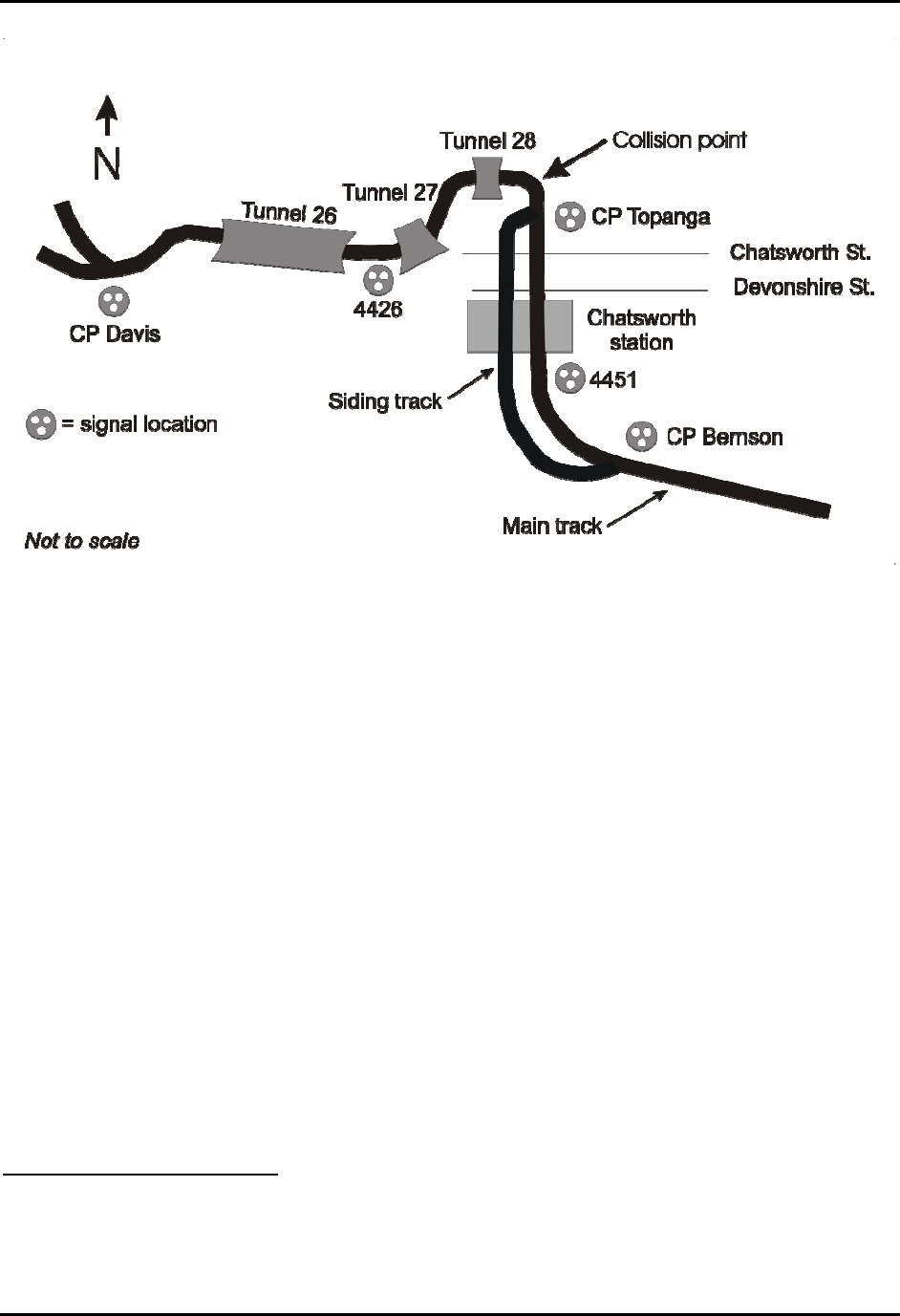
Figure 2. Accident site.
According to signal data logs, the next signal encountered by train 111 after CP Bernson
(intermediate signal 4451, just east [geographically south] of the Chatsworth passenger station
and the last signal before CP Topanga) was displaying a solid yellow approach
13
indication.
Train 111 passed signal 4451 at 4:18:41 p.m. Neither the engineer nor the conductor was
recorded calling out this signal indication.
At 4:20 p.m., Verizon Wireless network records logged a text message transmitted by the
UP conductor from his personal cell phone. At 4:20:15 p.m., a yellow-over-yellow approach
diverging
14
signal indication displayed at intermediate signal 4426, indicating to the Leesdale
Local’s crew that their train would be entering the siding at CP Topanga.
Train 111 stopped at Chatsworth station (about 1 mile east [geographically south] of CP
Topanga) at 4:19:20 p.m. The stop lasted 57 seconds. The conductor stated that once the train
stopped, he opened the train’s platform side doors and stepped down from the rear car onto the
platform to observe passengers stepping up and down from the train. The conductor stated that
his routine was to step back up to at least the first step of the rear passenger car before making
the final announcement of the train’s impending departure and pressing the buttons to close the
doors. He said the door closing sequence takes about 10 seconds, during which time the
conductor keeps the door open so he can look down the side of the train. In the first of his three
interviews with NTSB investigators, the conductor stated that when he looked forward alongside
13
Under an approach indication, trains are to “proceed prepared to stop at the next signal. Trains exceeding 40
MPH must begin reduction to 40 MPH as soon as head end passes signal.”
14
Under an approach diverging indication, a train must “proceed prepared to advance on diverging route at
next signal not exceeding prescribed speed through turnout(s).”
National Transportation Safety Board 5
NTSB Railroad Accident Report
the train, he could see a green (clear) signal at CP Topanga. (See figure 3.) In subsequent
interviews, the conductor stated that he had radioed the engineer to “highball 111 on a green
signal.”
15
Such an announcement was not recorded on any of the available recording devices. He
stated that he did not hear a response from the engineer.
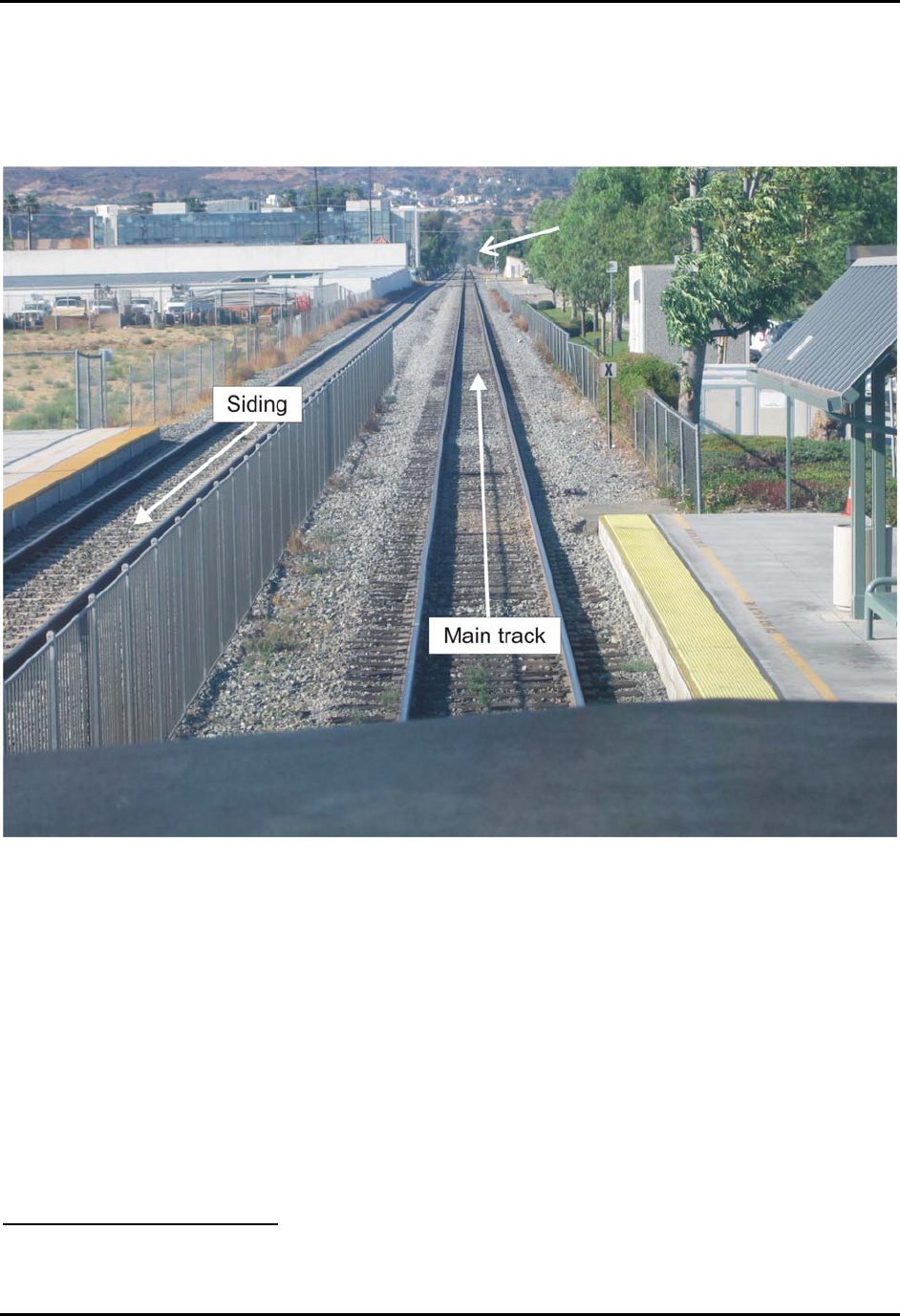
Figure 3. CP Topanga as viewed from the cab of a locomotive positioned at Chatsworth station.
Upper arrow indicates approximate location of the CP Topanga signal, which is about 5,288 feet
away.
Train 111’s event recorder showed that at 4:20:07 p.m., the engineer moved the throttle
from idle to position 2 and began releasing the train’s air brakes. At 4:20:13 p.m., the throttle
was moved to position 3. The conductor said that after he closed the crew door, he returned to his
desk to update his delay report. He said he had not heard the engineer call any signal since the
“green signals departing Northridge on our way to Chatsworth.” The data recorder indicated that
at 4:20:17 p.m., the brakes were fully released and the train speed was gradually increasing. At
4:20:19 p.m., the throttle was increased to its maximum position of 8, and train speed was 4 mph.
15
As will be discussed later in this report, several other individuals who were on the Chatsworth station
platform stated that as train 111 departed the station, they had seen the CP Topanga signal displaying a green aspect.
National Transportation Safety Board 6

NTSB Railroad Accident Report
National Transportation Safety Board 7
While departing Chatsworth station, the train remained under the operating authority of
the approach indication it had received at intermediate signal 4451. Under Metrolink rules,
engineers operating under this indication are not to exceed 40 mph while being prepared to stop
at the next signal. Additionally, Metrolink’s delay-in-block rule (Rule 9.9, discussed later in this
report), required engineers, after a station stop,
16
to keep train speeds below 40 mph and be
prepared to stop before reaching the next signal, until such time as the next signal can be seen to
display a proceed indication.
At 4:20:20 p.m., the engineer activated the locomotive bell for 42 seconds. At 4:20:51
p.m., he sounded the locomotive horn for 11 seconds for the Devonshire Road grade crossing. At
4:21:03 p.m., Verizon records show that the engineer received the seventh text message from
Person A. At 4:21:23 p.m., the engineer activated the locomotive bell for 19 seconds and also
made a short (1 second) sounding of the locomotive horn. While the bell was on, the engineer
began sounding the horn at 4:21:34 p.m. for the next crossing at Chatsworth Street. At 4:21:35
p.m. the train’s speed was 52 mph. The engineer stopped sounding the horn at 4:21:41 p.m. The
train’s speed had increased to 54 mph. Over the next 5 seconds, the engineer moved the throttle
first to 5, then to 6, back to 5, then to 7, then back to 3 and, finally, to throttle position 4.
At that time, train 111 was about 1,200 feet from the signal at CP Topanga. At 4:21:46
p.m., the engineer initiated a minimum brake pipe pressure reduction that slowed the train. The
train passed the CP Topanga signal at 4:21:56 p.m. traveling 44 mph. At 4:22:00 p.m., the
engineer released the train’s air brakes, and at 4:22:01 p.m., based on the time the transmission
was logged as received by the Verizon network, he sent his sixth text message to person A.
According to recorded data for the power-operated switch at CP Topanga (about 377 feet
west of the westbound Topanga signal), train 111 ran through the switch at 4:22:02 p.m.
17
At this
time, the train’s brakes were off and the throttle remained in position 4. A few seconds later, the
defect detector just west of the CP Topanga switch broadcast a “no defects” message indicating
that train 111 had passed the detector.
On the approach to CP Topanga, the eastbound Leesdale Local traversed two tunnels; the
first (tunnel 27) was 924 feet long, and the second (tunnel 28) was 547 feet long. Exiting the
second tunnel, the train entered a 6º right-hand curve. According to the Leesdale Local’s
crewmembers, as their train exited the second tunnel and entered the curve at 40 mph, the
Metrolink train came into view. The Leesdale Local’s crew activated the train’s emergency air
braking system, but the trains collided a few seconds later.
The collision occurred at 4:22:23 p.m., about 22 seconds after the Verizon network
logged receipt of the engineer’s last text message. The point of collision was 634 feet from the
east portal of tunnel 28. The event recorder indicated that the train 111 engineer made no change
in throttle position or brake application during the 21 seconds that elapsed from the time the train
ran through the CP Topanga switch until the collision occurred. Event recorder data indicated
16
The delay-in-block rule applied when a train was delayed for any reason, including a station stop, or
whenever train speed had been reduced below 10 mph.
17
The switch had been aligned for the eastbound Leesdale Local to enter the siding. Train 111 had “run
through” the switch from the opposite direction (against this alignment), which damaged the switch components.
NTSB Railroad Accident Report
that the Metrolink train was traveling about 43 mph and the Leesdale Local was traveling about
41 mph when the two trains collided head-on. (See figure 4.)
Emergency Response
The first 911 call about the accident was received by Los Angeles (City) Fire Department
Operations Control Dispatch at 4:23 p.m. from a nearby resident. The dispatch was initially
categorized as a “vehic” incident (a physical rescue assignment) but on the basis of numerous
additional calls, the incident was upgraded to a “derail” incident, which doubled the resources
dispatched.
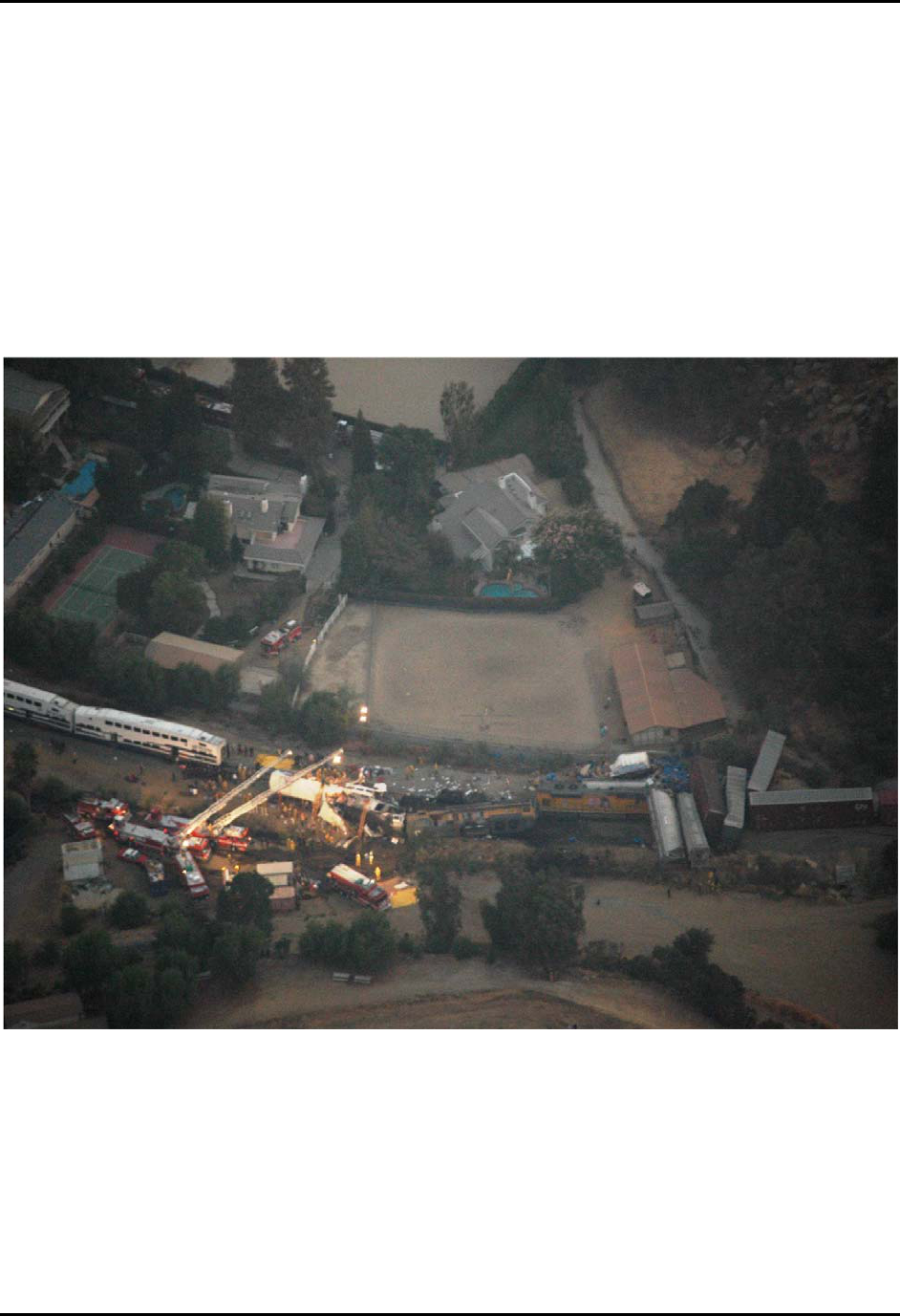
Figure 4. Overview of accident scene looking south.
The dispatch center requested resources from the Ventura County, Los Angeles County,
Culver City, and Beverly Hills fire departments. Los Angeles County Fire Department sent two
urban search and rescue teams and helicopters. Ventura County Fire Department sent advanced
life support rescues and two squads. Beverly Hills Fire Department and Culver City Fire
Department sent rescue squads.
The Los Angeles City Fire Department dispatched the department psychologist, critical
response teams, safety officers, and incident management teams. The critical response teams
National Transportation Safety Board 8

NTSB Railroad Accident Report
National Transportation Safety Board 9
provided family assistance. The incident management teams included fire department officers on
special duty, including a rail liaison officer.
The city fire department’s operations command was opened to coordinate with the
emergency operations center. The general manager of the Emergency Management Division
coordinated with different departments of the city to provide long-term logistics such as lighting,
food, and water.
Command, Organization, and Resources
The first responding companies were initially dispatched to a residential area near the
railroad. The first on-scene captain initially assumed charge of the incident and assigned fire
suppression, extrication, and medical tasks. A battalion chief then assumed command when he
arrived on scene and remained in charge until the arrival of the assistant chief.
The assistant chief initially established a command post in a school parking lot. When a
grassy field adjacent to the command post was selected as a helicopter landing zone, the
command post was moved to a parking lot farther away. During the course of the response, the
assistant chief established a fire suppression group, an extrication group, and a medical group. A
hazardous materials group was established to obtain the train consist and confirm the content of
the freight cars.
A unified command system was established with responding agencies. The Los Angeles
Police Department was in charge of security and perimeter control. Additional responding
agencies were the Los Angeles County Sheriff’s Department, Los Angeles County Fire
Department, Ventura County Fire Department, Metrolink, Union Pacific, California Office of
Emergency Services, the Los Angeles County Coroner, three private ambulance services, and the
Red Cross. Los Angeles city agencies that responded were the Department of Transportation, the
Department of Public Works, and the Unified School District. Metrolink’s chief of safety and
security was in charge of Metrolink’s response to the accident.
A fence separating the railroad property from the adjacent school was opened to provide
access between the trains and the command area. A medical triage area was established next to
this fence line. Because of the number of injured passengers, private ambulances were requested
to supplement the 28 fire department ambulances. Five air ambulances from Los Angeles Fire
Department, the Los Angeles County Fire Department, and the Los Angeles County Sheriff’s
Department responded. A total of 26 air ambulance flights were conducted. The fire
department’s medical director responded to the scene, along with two medical “caches” (trailers
stocked with medical supplies). During the first 8 hours of the response, the fire department
resources included 42 fire companies, 25 ambulances, 8 chief officers, 7 emergency medical
services captains, 3 urban search and rescue teams, 5 helicopters, 2 command post units, and 2
communications support units. In total, 350 firefighters (from all fire departments), 150 sheriff’s
department deputies, and 440 Los Angeles Police Department officers responded. In all, more
than 1,000 emergency personnel participated in the response effort.

NTSB Railroad Accident Report
National Transportation Safety Board 10
Extrication Operations
The earliest responders accessed the accident site from the rear yard of a house in the
adjacent residential area. The first police officers to arrive on the scene used bolt cutters to cut
through the fence and provide access to the accident site.
Leesdale Local. The Leesdale Local had two locomotive units, each with two exits. The
engineer and conductor were in the lead unit; the brakeman occupied the second unit. After the
collision, the second unit remained upright, and the brakeman was able to exit unassisted through
the rear cab door. Because the lead unit came to rest on its left side, the door on the right side of
the cab (behind the engineer’s seat) was too high for the crewmembers to reach. The second
door, through the nose of the unit, was blocked by the Metrolink locomotive.
As a result of the collision, a fire started that was fed by diesel fuel leaking from a fuel
tank that had separated from the Metrolink locomotive. The leaking fuel tank had come to rest
next to the occupied cab of the lead Leesdale Local locomotive. While efforts were underway to
suppress the fire, firefighters heard pounding coming from the lead locomotive cab. They looked
through the cab windows and saw that the two crewmembers were trapped inside. Firefighters
attempted to break the windshield and cut a front window, but neither effort was successful.
They were finally able to cut through the rubber molding around the window and remove it.
Upon removing the window, they found that the cab was filled with smoke.
According to the captain in charge of fire suppression, one of the crewmembers exited
the cab with severe back injuries. The captain helped him to the triage area. The second
crewmember was not able to move and could not exit the cab without assistance. Two
firefighters removed him from the cab and carried him to the triage area.
Metrolink Train 111. As firefighters set to work getting passengers out of the first
passenger coach, which was the most seriously damaged car, additional deputies and officers
from the California Highway Patrol began to arrive on scene. Firefighters working deeper into
the car began handing debris to the deputies and officers, who then removed the debris from the
car. As victims were removed from the wreckage, they were placed on backboards and carried
from the car by a line of deputies and officers. This activity at the first passenger coach
continued for 3 to 4 hours.
Meanwhile, teams were searching the second and third passenger coaches. A police
officer said that when he entered the second passenger coach, he saw that most of the passengers
had exited but that six people were still in the car and that they could not move. Three were on
the first level, and three were on the second level. Firefighters from the Los Angeles County Fire
Department next arrived at the second and third cars and began triaging the passengers. In the
third passenger coach were four or five passengers who received assistance.
Survivors removed from all of the cars were first taken to a patient holding area on the
north side of the train. As the patient numbers increased, they were moved to a patient collection
area farther away from the train. Law enforcement officers helped carry the backboards and
baskets used to move patients to the patient collection area. Chaplains began arriving on scene
and assisted fire department personnel. A temporary morgue was established to the side of the
wreckage.
NTSB Railroad Accident Report
National Transportation Safety Board 11
Firefighters sent to walk the UP train to check the train’s contents reported that they
found nothing of concern. A UP representative told responders where to find a copy of the train
consist, which the firefighters retrieved from the lead UP locomotive.
Fire department and railroad resources were coordinated through a city fire department
rail liaison officer working with Metrolink personnel. Overnight, Metrolink’s security
coordinator was placed in charge of the railroad’s response. Metrolink had staged heavy
equipment about a half mile away from the accident site. A UP representative also coordinated in
the arrival and staging of heavy equipment and equipment operators.
Battalion chiefs met periodically with representatives of the urban search and rescue
teams and the railroads to plan operations. Rescue efforts continued until about 1:00 a.m. on
September 13, at which time rescue operations transitioned to recovery operations. The
Metrolink locomotive was pulled away from the first passenger car about 8:00 a.m. on
September 13. Recovery operations continued until the final victim was recovered about 2:00
p.m. on September 13.
Injuries
Table 1. Injuries.
Injury Type Train Crews Passengers
Emergency
Responders
Total
Fatal
1 24 0 25
Serious
3 25 0 28
Minor
1 71 1 73
None
0 0 0 0
Total
5 120 1 126
Title 49 CFR 840.2 defines fatality as the death of a person either at the time an accident occurs or within 24 hours
thereafter. Title 49 CFR 830.2 defines serious injury as “an injury which: (1) requires hospitalization for more than 48
hours, commencing within 7 days from the date the injury was received; (2) results in a fracture of any bone (except
simple fractures of fingers, toes or nose); (3) causes severe hemorrhages, nerve, or tendon damage; (4) involves any
internal organ; or (5) involves second or third-degree burns, or any burn affecting more than 5 percent of the body
surface.”
Damage
The Metrolink train 111 locomotive sustained substantial crush damage in the collision,
with damage estimated as $3.5 million. The first passenger coach behind the locomotive was
destroyed, at a cost of $2.2 million. The remaining two Metrolink passenger coaches were
substantially damaged, with repair costs estimated as $1.5 million.
The UP estimated damages to the locomotives of the Leesdale Local as $1.2 million, with
an additional $2.123 million in damages to cars and $200,000 losses in lading. Cleanup expenses
were estimated as $500,000 for the UP and $670,000 for Metrolink. Damage to the track
structure was estimated as $250,000. Total damages were estimated to be $12.143 million.

NTSB Railroad Accident Report
National Transportation Safety Board 12
Personnel Information
Metrolink Train 111
The engineer and conductor of Metrolink train 111 at the time of the accident worked a
regularly assigned 5-day week, Monday through Friday, with Saturdays and Sundays off. The
crew had worked together on this assignment since April 15, 2008. The crew was scheduled to
arrive at Moorpark at 4:45 p.m. They would then operate train 118 from Moorpark, departing at
4:57 p.m. and arriving at Union Station at 6:20 p.m. The crew would then operate train 119 from
Union Station to Montalvo, departing at 6:40 p.m. and arriving at Montalvo at 8:35 p.m. They
would go off duty at 9:05 p.m. with an average total time on duty of 10 hours 37 minutes.
Engineer. The engineer of Metrolink train 111, age 47, was hired by Connex Railroad,
LLC,
18
(Connex) on June 25, 2005. Between November 1998 and June 2005, he had worked as
an engineer for Amtrak. Connex files disclosed no record of any formal disciplinary action with
regard to the engineer. The engineer’s record did show that he had received five “Letters of
Counseling” (considered informal discipline) in the previous 4 years. In December 2005, he was
counseled about his failure to report for duty on his assigned job. In December 2006, he was
counseled about his failure to report that his conductor was late for a job assignment. In August
2006 and again in December 2006, he was counseled about the number of times he had been
absent from work during the previous 12 months, a number that constituted a violation of the
Connex attendance policy. Two days before the accident, the engineer was counseled about his
responsibility for delaying train 119 on August 19, 2008, at Moorpark station. As will be
discussed in more detail later in this report, the engineer had, on two occasions, received oral
counseling about his cell phone use while on duty.
The engineer’s most recent recertification occurred on July 24, 2007 and was valid until
September 10, 2010. Connex records disclosed that the engineer had successfully completed his
last rules examination on May, 14, 2008. A check of the engineer’s work history revealed his last
missed workday was September 3, 2008, when he used an accrued personal day.
Time sheets provided by Connex showed that the engineer worked the same schedule for
the four days, Monday through Thursday, preceding the day of the accident. Under that schedule,
he went on duty at 5:54 a.m. at Montalvo. He departed on train 106 at 6:44 a.m. and arrived at
Los Angeles Union Station at 8:28 a.m. He was off duty from 9:26 a.m. until returning to work at
2:00 p.m. He departed Union Station westbound on train 111 at 3:35 p.m. and arrived at
Moorpark at 4:45 p.m. He departed Moorpark eastbound at 4:57 p.m. on train 118 and arrived at
Union Station at 6:20 p.m. At 6:40 p.m., he departed Union Station on train 119 and arrived at
Montalvo at 8:35 p.m. He went off duty at 9:05 p.m.
On the day of the accident, as on the previous 4 days, the engineer went on duty at 5:54
a.m. He operated a train from 6:44 a.m. until going off duty at 9:26 a.m. He returned to duty at
18
Connex Railroad, LLC, under contract to the SCRRA, provided the locomotive engineers and conductors for
Metrolink trains, along with the management, administrative, and training services required to support rail
operations.
NTSB Railroad Accident Report
National Transportation Safety Board 13
2:00 p.m. At 3:35 p.m., he departed on train 111. At the time of the accident, the engineer had
most recently been on duty for the second portion of his workday for about 2 hours 22 minutes.
Conductor. The train 111 conductor, age 57, was hired by Connex on June 25, 2005. He
was previously employed as a conductor by Amtrak beginning in March 1997. According to
Connex records, the conductor had successfully completed his last operational rules tests on May
13, 2008. Connex files disclosed no record of any formal disciplinary action with regard to the
conductor. The conductor received informal discipline in the form of a “Letter of Counseling”
regarding his responsibility for the delay of train 119 on August 19, 2008, at Moorpark station.
The conductor said that he had worked on the Monday and Thursday before the accident
and had been off on Tuesday and Wednesday. On each of his workdays, he awoke at 3:00 a.m.
and left for work at 4:00 a.m. He departed on a train at 6:44 a.m. and worked until 9:26 a.m.,
when he went off duty. He worked the second part of his day from 2:00 p.m. until 9:05 p.m. He
worked this same morning schedule on the day of the accident and was into the second portion of
his workday when the accident occurred. At that time, he had been on duty for the second
portion of his workday for about 2 hours 22 minutes, and awake for about 13 hours 22 minutes.
Union Pacific Leesdale Local
Three crewmembers (engineer, conductor, and brakeman) were on the Leesdale Local at
the time of the accident. This was the regular assignment for the engineer and brakeman; the
conductor was an extra-board
19
employee filling in for the regularly assigned conductor.
Engineer. The engineer, age 65, was hired by the UP railroad on April 3, 1969. UP files
disclosed no record of any disciplinary action pertaining to the engineer in the 2 years prior to
the accident. The engineer’s most recent recertification occurred on September 3, 2008. It is
valid until January 31, 2010.
The engineer stated that he arose every day between 6:00 a.m. and 6:30 a.m., departed his
residence for work at 10:30 a.m., and went on duty at 11:30 a.m. He said he usually went off
duty between 6:30 p.m. and 7:00 p.m.
20
He added he retired each evening no later than 11:30
p.m. At the time of the accident, he had been awake for approximately 10 hours and on duty for
just under 5 hours.
Conductor. The conductor, age 32, was hired by the UP Railroad on June 22, 1998. UP
files disclosed no record of any disciplinary action with regard to the conductor in the 2 years
prior to the accident.
The conductor said that he awoke about 9:30 a.m. on Monday, September 8. He went on
duty at 11:30 a.m. on the Leesdale Local, worked until about 6:30 p.m., and returned home. He
19
The extra board is a list of qualified employees available to fill in for regularly assigned workers or to work
non-scheduled assignments.
20
According to UP records, with the exception of Tuesday, September 9, when he went off duty at 6:55 p.m.,
the engineer went on duty at 11:30 a.m. and off duty at 6:30 p.m. each day beginning Monday, September 8, through
the day of the accident.

NTSB Railroad Accident Report
National Transportation Safety Board 14
said he retired for the evening between 11:00 p.m. and 11:30 p.m. He did not work the following
day, Tuesday, September 9, and awoke about 10:00 a.m. He retired for the evening about 11:45
p.m. He did not work the following day, Wednesday, September 10, and arose about 8:45 a.m.
He retired for the evening about 1:00 a.m. the following day, Thursday, September 11. He arose
later that day about noon, again did not work, and retired for the evening about 11:00 p.m. He
awoke the following morning, Friday, September 12 at 9:30 a.m. when he was called for duty.
He reported for duty at 11:30 a.m. to work the Leesdale Local. At the time of the accident, he
had been awake for about 6 hours 42 minutes and on duty for just under 5 hours.
Brakeman. The brakeman, age 64, was hired by the UP on January 2, 1965. UP files
disclosed no record of any disciplinary action with regard to the brakeman in the 2 years prior to
the accident.
The brakeman recalled that on Tuesday, September 9, and Wednesday, September 10, he
arose about 7:00 a.m., reported for work by 11:30 a.m., and went off duty about 7:00 p.m. On
both evenings, he retired by 9:30 p.m. He awoke at 6:00 a.m. on Thursday, September 11,
reported for duty at 11:30 a.m., and went off duty about 7:00 p.m. He retired for the evening
between 9:30 p.m. and 10:00 p.m. He awoke the following morning, Friday, September 12, at
6:00 a.m. and reported for duty at 11:30 a.m. At the time of the accident the brakeman had been
awake for almost 10 hours 30 minutes and on duty for just under 5 hours.
Person A
The individual referred to in this report as Person A is a teenager and a self-described
“rail fan.”
21
He said he has several friends who were also rail fans (two of whom are referred to
later in this report as “Person B” and “Person C”) and that he met the accident engineer in May
2008 through one of those friends. He said he would occasionally see the engineer at various rail
stations while he was watching trains and that the two would sometimes engage in brief
conversations centered around rail operations or the engineer’s career. The conversations were
brief, he said, “because [the engineer] would usually be driving the train, and he’d come in, you
know, say ‘Hi,’ and leave.”
Person A said that he would occasionally send text messages to the engineer while he
was on duty and that the engineer would respond “when he got a chance.” Person A recalled
having spoken to the engineer via cell phone about 12:30 p.m. on the day of the accident. He said
the engineer sounded “happy and cheerful, like I always remembered him to be.” He also
remembered that they exchanged a “few” text messages that morning, “because that was a very
busy shift for him.”
Person A recalled that after 3:35 p.m. on the afternoon of the accident, he received a text
message from the engineer about every 15 minutes. He said he sent the engineer a text message
shortly after 4:00 p.m. and received the last text message response from him at 4:22 p.m. He
recalled the message pertained to an Amtrak train that was running behind schedule.
21
A rail fan is an individual for whom railroading is a hobby. Rail fans may focus their interest on one or
several aspects of railroading, such as railroad history, locomotives, rolling stock, or overall train operations.

NTSB Railroad Accident Report
Person A said he was at home after receiving the text message at 4:22 p.m. and that he
had turned on the news sometime after that time and learned of the accident. He said that when
he heard that the accident had occurred at Chatsworth, he immediately knew it was the
engineer’s train, as it was the only Metrolink train that would have been there at that time.
Train and Mechanical Information
Metrolink Train 111
Metrolink train 111 consisted of one diesel-electric locomotive unit, two passenger coach
cars, and one passenger coach/cab control car. The locomotive was about 58 feet long, and each
of the cars was 85 feet long, for a total train length of 313 feet.
The first two passenger cars of the train were conventional coaches manufactured by
Bombardier Transportation Corporation (Bombardier) and delivered in the 2001-2002 time
frame. The remaining passenger coach was, at the time of the accident, operating as a
conventional passenger coach although it was also a cab control car with an operating
compartment from which the train was run when operating in the “push” mode (locomotive at
the rear). (See figure 5.) The cab control car was manufactured by the Urban Transportation
Development Corporation (UTDC) (now a part of Bombardier) and delivered in December 1992.
Both passenger coaches and the coach/cab control car are referred to as BiLevel coaches.
Figure 5. Bombardier BiLevel passenger coach of the type involved in this accident
National Transportation Safety Board 15
NTSB Railroad Accident Report
National Transportation Safety Board 16
The coach bodies were a semi-monocoque
22
construction that incorporates a non-linear
structural steel center sill element manufactured from a low-alloy high-tensile steel and an
aluminum alloy superstructure. Structural test reports indicates a delivery requirement that the
carbody structure resist a minimum static end (compressive) load of 800,000 pounds, as applied
on the centerline of draft, without any permanent deformation to any member of the car
structure. Collision posts are provided in the front bulkhead to help prevent carbody
telescoping.
23
Delivery documentation indicated that static end-load structural testing was
successfully conducted on an exemplar railcar representing each delivery series of cars involved
in this accident. The test results showed that the car structural design has been demonstrated to
satisfy the requirements of the Association of American Railroad’s Manual of Standards and
Practices and of 49 Code of Federal Regulations (CFR) 229.141(a), both of which include a test
requirement that the carbody structure resist a minimum static end (compressive) load of 800,000
pounds.
Although referred to as “bi-level” or “double-deck,” these coaches actually have three
separate levels of passenger seating accommodations. The design incorporates two full decks (an
upper and lower) in the center of the railcar, with an intermediate-level deck situated over the
truck assemblies at each end of the car. All three decks provide passenger seating. The BiLevel
coaches are all configured to the same basic passenger seating arrangement. The only significant
difference between a conventional coach and a cab control car is that the latter is equipped with
an operator’s cab compartment at its leading end. The cab control car can accommodate 142
passengers; the conventional coach seats 143. Both coach designs have a crush load
24
capacity of
about 360 passengers.
Two stairwells in each coach
25
provide access between the lower-level deck, the
intermediate level at each opposite end of the railcar, and the upper-level deck. Passengers enter
and exit the coaches through four main pneumatically operated pocket door sets
26
on the lower-
level deck of each railcar, with two sets of doors on each side. A vestibule area is provided
between the main side-exit doors at each end of the lower-level deck. An emergency release
handle adjacent to each main side-exit door may be used to release one of the sliding pocket door
panels at each door location. A restroom is at one end of the lower-level deck. A door at each
end bulkhead on the intermediate level provides passage to adjacent railcars.
22
In monocoque construction, the structural load is borne by the vehicle’s external skin rather than by an
internal frame. In semi-monocoque construction, internal bracing is added to supplement the load-bearing capability
of the vehicle skin.
23
Telescoping occurs when a railcar body breaches the end-structure of another carbody and passes into the
structure of that carbody, emulating a “telescoping” action. Telescoping can also occur when a single carbody is
placed under severe compressive axial loading that causes a localized structural failure with consequent partial
overlapping of the carbody sidewall panels.
24
The crush load is the maximum number of passengers that can possibly be riding in the railcar (standing and
sitting).
25
The stairwells are located approximately 1/4 of the car length from each end of the car.
26
A pocket door is a door that opens by sliding horizontally into a narrow compartment within the wall
adjacent to the doorway.
NTSB Railroad Accident Report
National Transportation Safety Board 17
Passenger seating accommodations on board the Metrolink BiLevel railcars consist of a
combination of transverse and longitudinal-mounted fixed seat assemblies,
27
with the seat
assemblies installed on both sides of a longitudinally oriented center aisle passageway on all
three deck levels. Almost all of the transverse mounted fixed seat assemblies in the Metrolink
BiLevel coach railcar fleet are arranged in a “2+2,” paired/side-by-side configuration (also
referred to as a “paired seating sets” arrangement). Many of the paired seating sets are arranged
in an opposing face-to-face layout with the balance of the paired seating sets arranged so that the
paired seating sets are all facing in the same direction.
Each Metrolink BiLevel railcar is equipped with eight workstation tables, four on the
upper level and two at each end of the intermediate level. These tables are fitted between paired
seating sets of opposing passenger seats. The tables are a basic design consisting of a one-piece
tabletop assembly that is cantilevered from the carbody sidewall and supported by a single
pedestal leg. The tabletops are trapezoidal in shape, approximately of a uniform size, and
manufactured of a high-pressure laminate without any form of safety padding.
Inspections and Maintenance. An examination of inspection and maintenance history
records for each of the Metrolink cars and the locomotive unit involved in the accident revealed
that the equipment had received all required inspections and scheduled maintenance.
Postaccident Inspections. Investigators inspected the rear two Metrolink cars at the
accident site and tested the air brake system.
28
The air brake system on the cars was charged to
111 pounds per square inch (psi), then a 20-psi reduction was made and a leakage test conducted.
The cars had 2-psi-per-minute brake pipe leakage.
29
The air pressure reduction caused all the
train tread and disc brakes to apply as designed. All the contact surfaces were smooth and work-
polished.
The brake pipe was recharged (pressurized), and the brake shoes released. An emergency
application (a rapid reduction of brake pipe pressure to 0 psi) was then initiated from the
locomotive unit. The brakes at each location again applied; however, the disc brake at one
location on the cab control car subsequently released. The actuator at that location was found to
be loose and moved more than normal when shaken by hand.
The air brake systems on the Metrolink locomotive unit and first car were damaged in the
accident to the extent that no meaningful test could be performed. The contact surfaces of both
were inspected and found to be smooth and work-polished. The front truck on the locomotive
unit had thermal cracking at several sites around the circumference of the wheels.
27
A fixed seat is a passenger seat that is permanently configured in a given location such that it cannot
otherwise be readily reconfigured (by operational or maintenance personnel) to face any other direction.
28
Train brakes are activated using air pressure maintained in the “brake pipe,” a continuous pipe extending
from the locomotives to the last car in a train when all cars and their air hoses are coupled. (The term “brake pipe” is
also used when referring to a single car.) A reduction in brake pipe pressure causes the brake shoes on each car to
apply, with the degree of application proportional to the amount of the pressure reduction. When the reduction is
stopped and brake pipe pressure increases, the brakes release.
29
Federal Railroad Administration regulations (49 Code of Federal Regulations 238.313) allow up to 5-psi-per-
minute leakage so long as such leakage does not affect service performance.

NTSB Railroad Accident Report
National Transportation Safety Board 18
Event Recorders. The Metrolink locomotive unit was equipped with an event recorder
that sustained significant thermal and crush damage in the accident. The damaged recorder was
recovered and sent to the NTSB’s Vehicle Recorders Laboratory in Washington, D.C., where
investigators removed its memory module. On September 18, 2008, an NTSB investigator took
the module to the recorder’s manufacturer, Bach-Simpson, where the recorded data were
successfully downloaded. The Metrolink cab control car (the last car of the train in this accident)
also had an event recorder. This recorder was undamaged in the accident, and investigators
downloaded its data on scene.
Leesdale Local
The UP Leesdale Local consisted of two diesel-electric locomotive units and 17 cars (7
loads and 10 empties). The train, including the locomotive units, weighed 1,523 tons and was
1,164 feet long.
Postaccident Inspections. The rear seven cars from the Leesdale Local were inspected at
Moorpark, California, on Sunday, September 14, 2008. The air brake system on the cars was
charged to 90 pounds per square inch, gauge, (psig), then a 20-psi reduction was made and a
leakage test conducted. The cars had 1/2-psi-per-minute brake pipe leakage, which was within
Federal allowable limits. When the brake pipe pressure was reduced, the brakes applied at each
location, as expected. When the brake system was recharged, all the brake shoes released
normally except for those at one location where a new wheel was evident.
Event Recorders. The Leesdale Local had event recorders on both locomotive units.
Data from the event recorder on the second unit was downloaded at the scene. Data from the
recorder on the lead unit could not be downloaded on scene;
30
therefore the recorder was sent to
the NTSB’s Vehicle Recorders Laboratory in Washington, D.C. On September 28, 2008, with
the assistance of the locomotive’s manufacturer, data from the lead unit event recorder were
successfully downloaded.
Video Recorders. The Leesdale Local locomotives were also equipped with
Wabtec/March Networks VideoTrax digital video recording device. These devices record audio,
video, and some parametric data. The video cameras were mounted to provide a forward-facing
view through the locomotive window. Black-and-white 720 x 480-pixel images are stored at a
rate of 15 per second. A microphone captures sound from outside the locomotive cab. GPS
time/date, position, and speed are captured along with horn and pneumatic control switch status
(on or off). The recorders can store approximately 80 hours of video/audio/data on a 60 Gb
removable hard disk. The video cameras on both locomotive units were sent to the UP playback
station in Omaha, Nebraska, where an NTSB investigator coordinated retrieval of the
information.
30
Locomotive event recorder data are typically downloaded while the recorder is installed in the locomotive
and the unit is running. Damage to the lead unit of the Leesdale Local prevented this method of data retrieval.

NTSB Railroad Accident Report
National Transportation Safety Board 19
Wreckage
Because of the urgent need to conduct rescue operations for passengers of the Metrolink
train, the accident site was significantly disturbed before NTSB investigators arrived on the
scene. During the rescue and recovery efforts, some of the derailed railroad equipment was
moved a short distance from where it initially came to rest and was available for examination.
Investigators used map graphics (based on aerial photographs) as well as aerial and ground-based
photographs to document the condition and location of this equipment before it was relocated.
For the railroad equipment that had not been disturbed or relocated, investigators were able to
examine and record observations of the physical aspects of the accident scene. The information
in the remainder of this section is based on this combination of documentation and direct
examination.
Metrolink Train 111
The three Metrolink passenger coaches remained where they initially came to rest,
although certain components of the lead passenger coach had been disturbed during the efforts to
extricate passengers. For example, much of the carbody side and roof panels and many of the
interior components (seats, floor, partitions, hand-hold stanchion posts) had been placed
temporarily in a debris pile immediately adjacent to where the railcar initially came to rest.
The other derailed railroad equipment, which included the Metrolink locomotive and
almost all of the UP equipment, had been moved but remained available for subsequent post-
recovery examination.
Locomotive. The Metrolink locomotive, which had been operating in a cab-forward
orientation, came to rest on its right side (relative to its normal direction of travel) with the
locomotive carbody longitudinally oriented roughly parallel to the track centerline. Obvious
severe collision impact damage was evident on the front end, both side panel areas, the
operator’s cab, and aft end of the locomotive. The locomotive’s front end was firmly wedged
against the front end of the lead UP locomotive, and its aft end penetrated the leading bulkhead
panel of the passenger coach to which it was coupled. The rear portion of the locomotive came to
rest within the confines of the occupant compartment of that first passenger car. In this position,
the locomotive carbody occupied approximately 52 feet, or approximately the forward two-
thirds, of the passenger coach. (See figure 6.)
NTSB Railroad Accident Report
Figure 6. The force of the collision drove the Metrolink locomotive about 52 feet into the
passenger space of the first coach behind the locomotive.
The operator’s cab, which had been occupied solely by the train engineer, sustained a
complete loss of survivable space. Post-recovery measurements of the locomotive indicated that
the front and rear ends of the unit had been compressively displaced by about 15 feet and about 1
foot, respectively. The locomotive had thus, as a result of the collision, compressed from its
original 58-foot length to a length of about 42 feet.
The fuel tank separated from the locomotive and was found resting on the track ballast a
short distance to the right side of the track, approximately adjacent to where the front of the
locomotive came to rest. The tank was breached and lost some of its contents of diesel fuel,
which burned in a fire.
The lead power-truck assembly had separated from the locomotive and was found resting
upright, close to the centerline of the track approximately adjacent to the mid-point of where the
lead UP locomotive had come to rest. The aft power-truck assembly remained attached to the
locomotive.
First Passenger Coach. The first passenger coach aft of the locomotive sustained severe
structural damage that compromised its occupant survivable space. According to the on-scene
emergency responders and representatives of the Los Angeles County coroner department, of the
24 passengers that were fatally injured in the accident, 22 were in this coach at the time of the
collision. One fatally injured passenger was determined to have been in the second passenger
National Transportation Safety Board 20

NTSB Railroad Accident Report
National Transportation Safety Board 21
coach, and the location of the other fatally injured passenger at the time of the collision could not
be determined. The car showed no evidence of fire damage.
As a result of the collision, the passenger coach derailed and came to rest at the
immediate right side of the track leaning severely toward its right side. Because of the
penetration of the aft end of the locomotive through the leading bulkhead panel, the forward one-
quarter of the coach (encompassing the intermediate-level passenger compartment, which is
above the lead-end truck) separated at the center sill and telescoped into the carbody, along with
the lead truck, which remained attached to this section of the car. The telescoping action purged
the entire interior carbody content in the forward two-thirds of the car such that only the outer
sidewalls, which had bulged and peeled outward, and roof structure of the carbody shell
remained. Within this area, the leading-end intermediate-, the lower-, and the upper-level
passenger compartments sustained a complete loss of occupant survivable space. The aft
intermediate-level passenger compartment (located above the aft-end truck), including the spaces
of the aft stairwells, were generally undamaged.
The aft truck assembly had separated from the car and was found resting upright on the
track ballast immediately adjacent to its normal location on the car frame.
The coupler shank at the aft end of the car was fractured and bent downward. The coupler
head had separated from the shank, which caused this car to separate from the second passenger
coach. The separation distance between the two cars was about 32 feet.
Second Passenger Coach. The second passenger coach from the locomotive did not
sustain severe structural damage in the accident, nor was its occupant survival space significantly
compromised. Only one of the fatally injured passengers was identified as having been
occupying this car at the time of the collision.
Investigators were able to examine this car before it was moved from its original
postaccident position. The car did not derail and came to rest in its normal orientation on the
track. The car showed some interior damage and several ripples along the exterior carbody, but it
exhibited no obvious exterior or interior catastrophic collision impact damage. The interior
damage consisted primarily of fractured seatbacks, dislodged seats, bent and separated stanchion
(vertical handhold) posts, dislodged or separated slider door and utility compartment panels,
dislodged or separated work-station tables, and dislodged or separated ceiling panels. The car
showed no evidence of fire damage.
A number of emergency windows had been removed by emergency responders. The
coupler shank at the leading end was fractured and bent upward, and the coupler head still
engaged the aft coupler head of the first passenger coach. At its aft end, the car remained coupled
to the third passenger coach.
Third Passenger Coach. The third passenger coach, although equipped as a cab control
car, was operating as a conventional coach at the time of the accident. Investigators were able to
examine this car before it was moved from its original postaccident position. The car did not
sustain severe structural damage during the collision, nor was its occupant survival space
significantly compromised. The car showed no evidence of fire damage.

NTSB Railroad Accident Report
National Transportation Safety Board 22
The car, which had been operating B-end forward, did not derail and came to rest in its
normal orientation on the track. The car showed no evidence of exterior or interior catastrophic
collision impact damage. The interior damage was similar to that exhibited by the second
passenger coach, including emergency windows that had been removed during the response.
UP Leesdale Local
Lead Locomotive. Damage to the lead locomotive of the UP train consisted primarily of
extensive frontal damage and some fire damage. No loss of occupant survival space in the
locomotive cab occurred.
Trailing Locomotive. The trailing locomotive had been disturbed from its immediate
postaccident condition and relocated. As a result, no detailed assessment could be made of the
damage the unit sustained during the collision. According to UP officials who were on the scene
immediately after the accident, damage to the unit consisted primarily of substantial distortion to
the roof of the operator’s cab. A segment of the roof panel had apparently been struck by a
derailed freight car during the collision.
Topanga Switch
Investigators examined the power switch machine at CP Topanga and found the switch
points split in mid-stroke, indicating that the switch had been run through in the trailing
position.
31
(See figure 7.) Additional visual inspection revealed that the throw-rod, basket rod,
and switch machine internal throw-rod were bent and damaged. Because of the nature and extent
of the damage, Metrolink signal personnel had to replace the switch machine.
Meteorological Information
The Van Nuys surface weather station, about 6.2 miles east of Chatsworth, reported
weather conditions at 3:51 p.m. on September 12, 2008, as follows: daylight, clear skies, haze,
calm winds, and a temperature of 73° F with visibility of 4 miles.
Track Information
The main track preceding CP Topanga generally consists of 136-pound continuous
welded rail.
32
The rail is seated in 16 by 7 3/4-inch double shoulder tie plates that lie between the
31
Switch points are the movable, tapered rail sections that are moved either against or away from the stationary
(stock) rail to allow a train to continue straight through the switch or to be diverted by the switch onto another track.
Trains approaching the switch from the side with the tapered switch points are said to be making a “facing point”
movement. Trains approaching from the opposite direction are making a “trailing point” movement.
32
Continuous welded rail (CWR) consists of rail sections that have been welded together in lengths greater
than 400 feet.

NTSB Railroad Accident Report
bottom surface of the rail and the top surface of timber crossties. The rail is fastened through the
tie plates to standard timber crossties with four lag screws, two on the gauge side (between the
rails) and two on the field side (outside the rails). A 6° curve begins just west of the Topanga
switch. Beginning at this point, the crosstie type changes from wood to concrete.
Figure 7. CP Topanga switch looking east, in the direction the Leesdale Local was traveling.
Circles highlight damage to switch points and components consistent with the switch having
been run through in a trailing point movement by the Metrolink train traveling in the opposite
direction.
In the wooden crosstie section, the ties are predominantly box anchored (four rail anchors
per crosstie, two rail anchors applied to each rail, a rail anchor on each side of a crosstie) with
rail anchors applied to every crosstie. The rail in the concrete tie sections is anchored on every tie
with two elastic fasteners. Both areas of track are supported by a mixture of semi-angular granite
ballast that fills the crosstie cribs. The depth of the ballast was estimated at 20 to 22 inches. The
ballast shoulders measured 20 inches wide on tangent (straight track) and 24 inches wide in the
curve. Investigators did not observe any fouled ballast conditions.
The Topanga switch itself is constructed of continuous welded rail, with the switch point
area completely welded (without rail joints). The switch uses Samson switch points and stock
rails that are beveled for a protected fit of the switch point against the stock rail.
National Transportation Safety Board 23

NTSB Railroad Accident Report
National Transportation Safety Board 24
Leading up to CP Topanga westbound, the maximum authorized speed is 70 mph for
passenger trains, which requires that the track be maintained to Federal Railroad Administration
(FRA) class 4 standards. Between CP Topanga and tunnel 28, a permanent speed restriction of
40 mph is in effect because of the 6° curvature in the track. Because of the lower maximum
speed, this track is maintained to FRA class 3 standards.
Signal Information
General
Control points on the Ventura Subdivision between CP Davis and CP Bernson are
equipped with Vital Harmon Logic Controller processors, and intermediate signals are equipped
with Electro-Code 4 processors, both of which are provided by General Electric Transportation
Services.
The Metrolink centralized traffic control system between CP Davis and CP Bernson uses
Safetran V-20 Colorlight signals and GRS Sentinel signals. The system uses US&S M-23A low-
voltage power-operated switch machines. Signal track circuits are controlled by Electro Code 4
electronic coded track circuits between control points and d.c. track circuits within control point
sections. Signals are arranged for movement in either direction.
Until the dispatcher has selected and cleared a route for a train, or trains, the signals at
either side of a control point are set to display a red aspect. Once the dispatcher has requested a
route that is not precluded by existing train traffic, the signals governing that route change to
display the appropriate aspects.
The Metrolink Operations Center uses the Digicon computerized dispatching system to
align routes for train movements. To facilitate traffic flow, dispatchers will often plan a sequence
of train movements in advance and then “stack” requests for those routes in the Digicon system.
The Digicon system will place those stacked requests in a queue and carry them out, in the order
in which they were entered, as train movements allow. For example, on the day of the accident,
the dispatcher selected the first route, which called for the eastbound Leesdale Local to proceed
from CP Davis along the main track and through the siding at CP Topanga. Before this move
could be completed, the dispatcher requested a second routing, which would allow train 111 to
proceed westbound on the main track through the switch at CP Topanga. Because the first route
the dispatcher had selected (for the Leesdale Local) took precedence, the request regarding train
111 was placed in the queue within the Digicon system. The Digicon system was designed to
carry out this request—which involved realigning the Topanga switch for the main line and
displaying a clear indication on the westbound Topanga signal—only after the Leesdale Local
was in the siding and clear of the main track. Until then, the design of the Digicon system
prevented it from transmitting the dispatcher’s route commands for train 111 to the appropriate
Harmon Vital Logic Controllers in the field. The logic circuits within the controllers are also
designed not to allow conflicting or opposing routes. That is, once the switches are set for an
eastbound train to move into the siding, the system will not (because of the interrupted electrical
circuit caused by the movement of the switch) allow the westbound signal at CP Topanga to
show any aspect other than red.

NTSB Railroad Accident Report
National Transportation Safety Board 25
Some of the signals on the Ventura Subdivision, including the signals at CP Topanga, are
“approach lit,” meaning that they will display a signal aspect only when a train enters the
segment of track governed by that signal. At other times, the signals are in the “conservation”
mode and remain dark as a way of reducing maintenance and extending the life of the signal
lamps. Thus, even though the signal circuitry of the westbound CP Topanga signal called for a
stop indication at the time of the accident, the red aspect of the signal did not actually illuminate
until train 111 passed intermediate signal 4451, just east of the Chatsworth station, at 4:18:41
p.m.
Review of Recorded Signal Data
Downloaded data from Digicon event logs at the Metrolink dispatching center and signal
event recorders in the field indicate that, at the time of the accident, the westbound signal at CP
Topanga was displaying a red aspect (stop indication) and the dispatcher’s stacked request to
clear this signal was waiting in the queue in the Digicon dispatching system.
The data logs for each signal reflect the aspect being displayed at any given time by a
notation in the log indicating which (if any) repeater relays for the various aspects are energized.
Because the current to energize the relay coil must pass through the lamp (light bulb) of the
aspect, the relay can only be energized (which moves the relay armature to the “up” position) if
the lamp for that aspect is intact and that current is flowing through it. If the lamp is not
energized, or if the bulb is burned out, the armature of the repeater relay for that aspect will be in
the “down” position. Signal event recorder logs for the westbound Topanga signal showed that
as train 111 approached the westbound Topanga signal, the armature of the repeater relay for the
red aspect was in the “up” position, indicating that the aspect was energized; the relays for the
yellow and green aspects were down and therefore not energized.
Operations Information
General
The SCRRA is the joint powers authority that oversees the Southern California commuter
rail service known as Metrolink. The system comprises 7 rail routes, 56 stations, and 512 total
route miles of track in six counties. Metrolink owns 37 locomotives and 135 commuter coaches
and leases additional coaches. The system transports about 45,000 passengers each day.
The accident occurred at milepost 444.12
33
on Metrolink’s Ventura Subdivision, about 33
miles west of Los Angeles. Timetable direction is east–west. This part of the subdivision features
a single main track. All train movements are governed by wayside signal indications of a traffic
control system administered from Metrolink’s operations center in Pomona, California. A
dispatcher at the operations center directly controls switches and signals at control points. (See
33
Milepost numbers decrease from east to west.
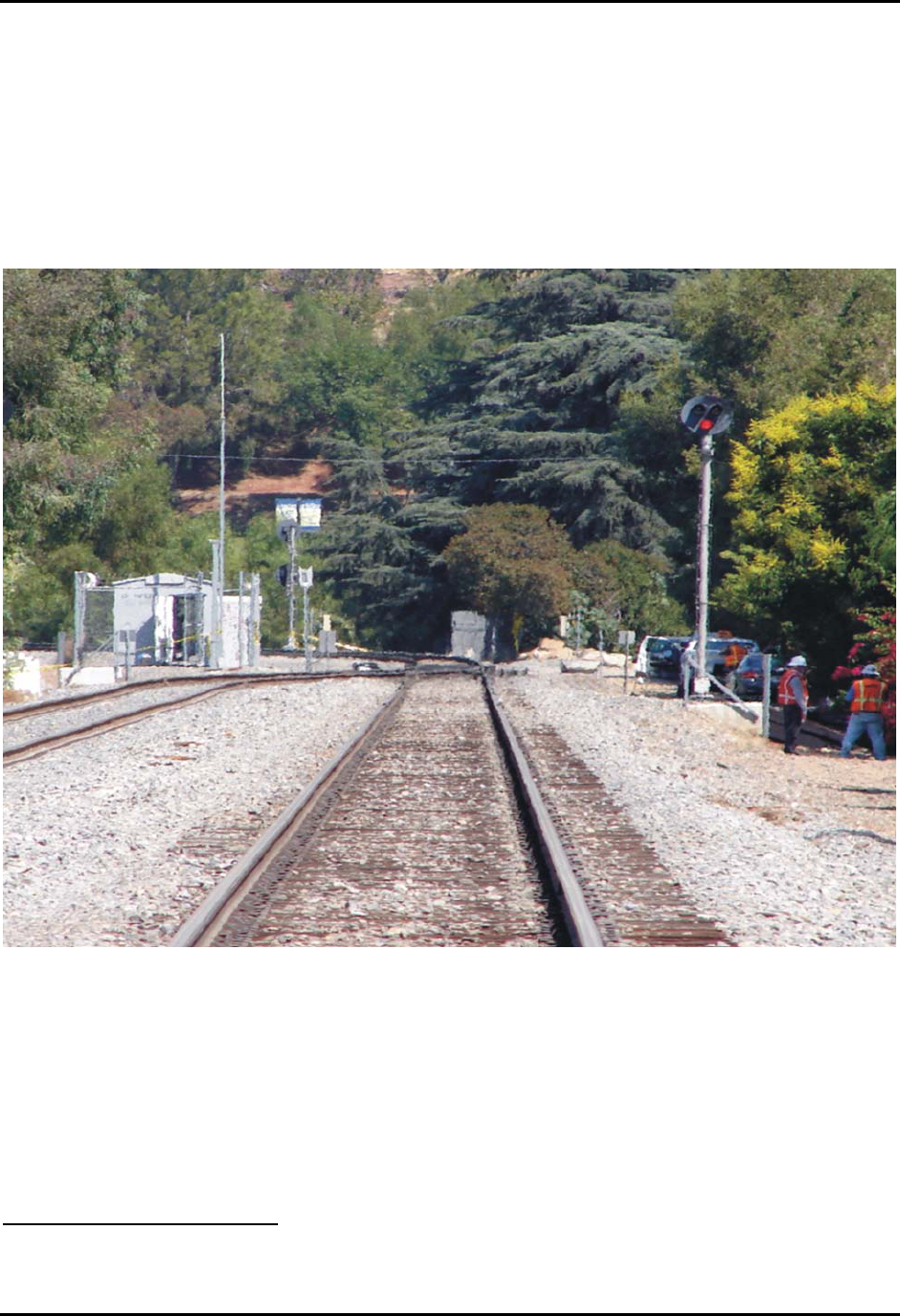
NTSB Railroad Accident Report
figure 8.) Between control points, intermediate signals automatically display the signal
indications appropriate for the existing track and traffic conditions.
Trains operate in both directions on the single track main line, with the subdivision
averaging 6 freight trains, 18 Metrolink trains, and 12 Amtrak trains daily. Maximum speeds are
60 mph for freight trains and 79 mph for passenger trains. Because of the curvature of the track
in the area of the accident, maximum allowable speed (between mileposts 442.6 and 444.5) is 40
mph.
Figure 8. Westbound signal at CP Topanga displaying a red aspect (indicating stop.)
Transportation services and operating crews are provided by transportation contractor
Connex.
34
On June 25, 2005, Connex entered into a 5-year contract with SCRRA to provide
Metrolink with operating crews, management personnel, and training support. These services had
previously been provided by Amtrak.
34
Connex Railroad, LLC, is a unit of Veolia Transportation, Inc., which entered the U.S. transportation market
in 2001.
National Transportation Safety Board 26

NTSB Railroad Accident Report
National Transportation Safety Board 27
Operating Rules and Efficiency Testing
Train operations on the Metrolink system are governed by the General Code of
Operating Rules, 5th edition, effective April 13, 2005, and by timetable and special instructions,
supplemented by Metrolink’s Manual of Instructions effective 12:01 a.m. on September 1, 2007.
Each railroad, under Title 49 CFR Part 217, “Railroad Operating Rules,” must carry out a
program of operational tests and inspections (efficiency tests) of operating crewmembers. The
Metrolink efficiency testing program, administered by Connex, became effective on June 26,
2005. The program was revised on July 1, 2008.
Under the program, tests were to be spread out and not confined to specific times and
days of the month. The tests were to include Metrolink and foreign line crews operating over
SCRRA property. At least half of the tests were to be on operating rules and special instructions.
Testing methods included visual observation, monitoring of live and previously recorded radio
and telephone transmissions, scrutiny of locomotive event recorder data, and use of radar or
other approved wayside speed monitoring devices.
Medical and Toxicological Information
A review of the Metrolink engineer’s railroad medical records showed that he had been
diagnosed with type 2 diabetes and was being treated with multiple medications, including less-
than-maximum doses of metformin, glipizide, and pioglitazone. The engineer also had high
blood pressure, which records showed was being effectively controlled by use of the prescription
medication benazepril. The engineer had been diagnosed HIV (Human Immunodeficiency Virus)
positive about 2 years before the accident. He was being treated with anti-retroviral medications,
which he was noted to be tolerating “very well with no side effects.” These HIV diagnosis and
retroviral medications had not been reported to the railroad medical department. Laboratory
evaluation dated September 3, 2008 noted that the virus was not detected in the engineer’s blood.
On July 6, 2007, an “Authorization to Work with Medication(s) and Without Work
Restrictions” completed by the engineer’s endocrinologist noted that the engineer was “fit for
duty and can complete all duties of the position.” The HIV diagnosis and antiretroviral
medications were not noted on this form.
One month before the accident, the engineer’s weight was recorded as 254 pounds. His
height was recorded as 6 feet during a company physical examination in 2005. In December
2004, records of a physician visit noted that the engineer “may have sleep apnea, but he has no
way of knowing. He thinks he does snore a lot ….” The autopsy report on the engineer noted that
his heart weighed 430 grams and that “All chambers are dilated.”
Pursuant to 49 Code of Federal Regulations (CFR) 219, Subpart C, “Post-Accident
Toxicological Testing,” toxicological specimens were obtained from the engineer and conductor
of the Metrolink train and from the engineer, conductor, and brakeman of the Leesdale Local.
The specimens were screened for cannabinoids, cocaine, opiates, amphetamines,
methamphetamines, phencyclidine, barbiturates, benzodiazepines, and ethyl alcohol. Tests
results for the Metrolink engineer and conductor and the Leesdale Local engineer and brakeman
NTSB Railroad Accident Report
National Transportation Safety Board 28
were negative for alcohol and the aforementioned drugs. The Leesdale Local conductor tested
positive for cannabinoids (marijuana) in both blood and urine and negative for alcohol.
35
Test
documentation indicated that the conductor’s blood and urine specimens had been taken at 1:30
a.m. on September 13, 2008, the morning after the accident.
Remaining portions of the specimens obtained from the Metrolink engineer and
conductor were sent to the Civil Aerospace Medical Institute (CAMI) in Oklahoma City,
Oklahoma, for independent and broader toxicological analyses. In those tests, the Metrolink
engineer tested positive for benazepril
36
and pioglitazone
37
in the blood and urine. The Metrolink
conductor tested positive for fluoxetine
38
and norfluoxetine
39
in the blood and urine and for
morphine (which had been administered during postaccident medical treatment) in the urine. The
conductor’s most recent physical examination had taken place in January 2006. At that time, the
conductor had reported using fluoxetine, and his medical examination report had been reviewed
and approved by the appropriate Connex authorities.
Asked about his positive test results, the Leesdale Local conductor stated that he had
smoked marijuana “three times at most” in July and August 2008, saying that those occasions
were his first use ever. He said he had not used marijuana on the day of, or several days before,
the accident.
Metrolink Engineer’s Use of a Wireless Device
Based on Verizon Wireless records, at the time of the accident, the Metrolink train
engineer was in possession of an LG Model VX10000 “Voyager” wireless device (figure 9).
40
Among its features, the device is capable of browsing the Web, sending and receiving e-mail and
text messages, downloading and playing music and video files, and capturing still images or
video.
As part of this investigation, the NTSB obtained Verizon Wireless records for the
Metrolink engineer’s account covering the day of the accident as well as the previous 28 days.
These records included the time and date of incoming and outgoing telephone calls as well as the
time and date of any text messages sent or received, picture/video messages sent or received, and
use of the device’s Web browser.
The records indicate that between 6:05 a.m. and 4:22 p.m. on the day of the accident, the
engineer sent or received a total of 95 text messages. During the time he was responsible for
35
Results indicated the blood specimen contained 13.7 nanograms per milliliter (ng/ml) of carboxy-THC (the
metabolite of the active ingredient of marijuana), tetrahydrocannabinol (THC), and 1.1 ng/ml of THC. The urine
specimen contained 117 ng/ml of carboxy-THC.
36
Benazepril is a prescription medication used to treat high blood pressure.
37
Pioglitazone is a prescription medication used to treat type 2 diabetes.
38
Fluoxetine (trade name Prozac) is a prescription medication used to treat depression, obsessive-compulsive
disorder, some eating disorders, and panic attacks.
39
Norfluoxetine is a metabolite of fluoxetine.
40
Investigators were not able to locate the engineer’s wireless device after the accident.
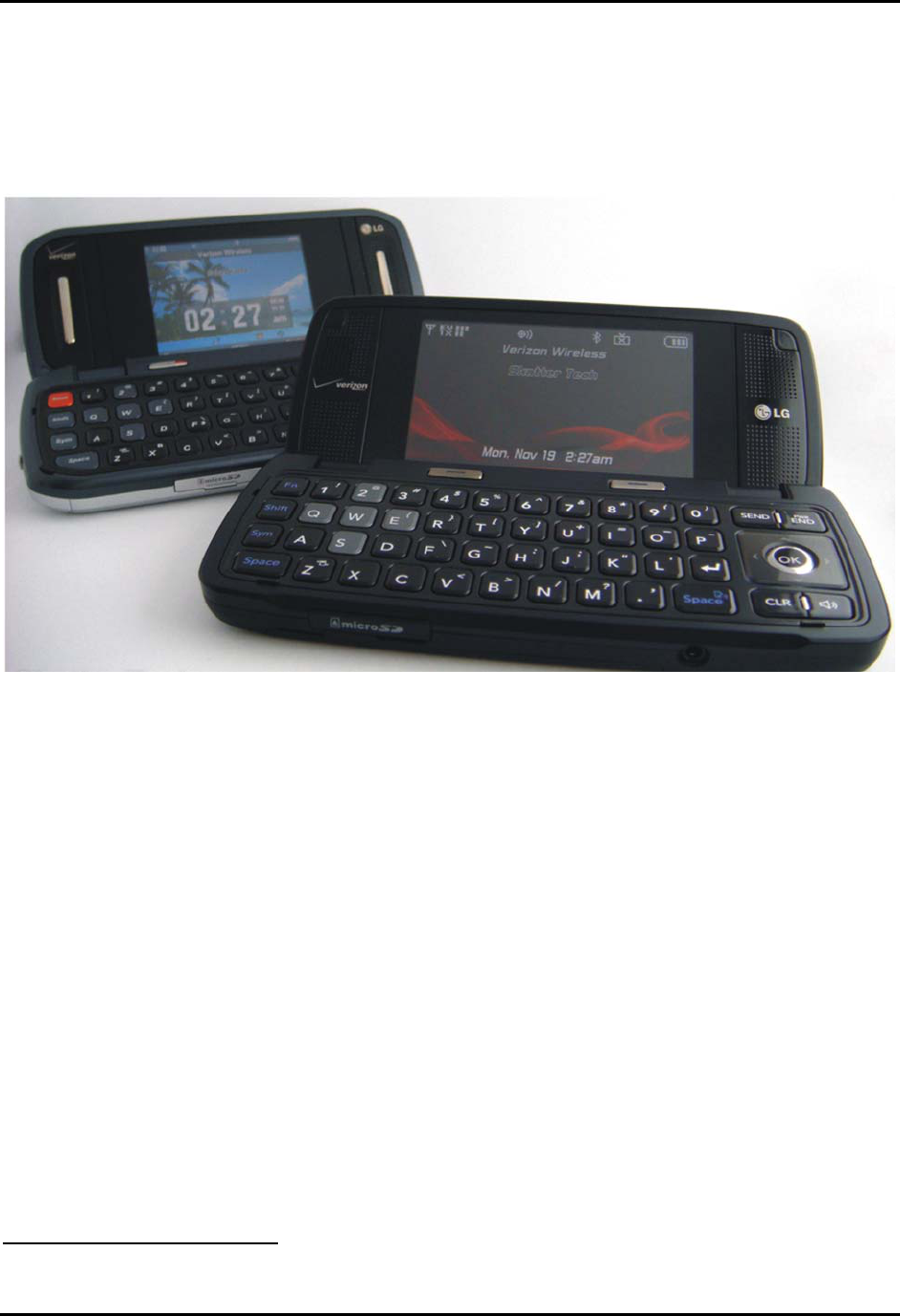
NTSB Railroad Accident Report
operation of a train (morning and afternoon shifts), the engineer sent 21 text messages, received
21 text messages, and made four outgoing telephone calls. The records show no picture message
activity on the day of the accident, and Verizon representatives told investigators that their
records showed no Web activity or use of “data services” by the engineer’s wireless device on
the day of the accident.
41
Figure 9. LG wireless device Model VX10000 similar to the device used by the Metrolink
engineer on the day of the accident. (Internet photograph)
The engineer began his morning shift on the day of the accident by moving train 106 out
of the Montalvo station storage yard at 6:25 a.m. He operated the train in revenue service from
6:44 a.m. until arriving at Los Angeles Union Station at 8:25 a.m. He then operated in non-
revenue service from Union Station to the central maintenance facility, arriving at 8:53 a.m.
During these times, he sent 15 text messages, received 15 text messages, and made two phone
calls (one lasting for 2 minutes 29 seconds, the other for 8 seconds). On the afternoon of the
accident, as previously noted, the engineer sent six text messages and received seven during the
time he was responsible for operating a train.
Pattern of Wireless Device Use
Investigators acquired the engineer’s daily time tickets for the week before the accident
and compared them with his cell phone records to determine whether the messaging activity on
41
Because the device was not recovered, the contents of its internal memory could not be accessed.
National Transportation Safety Board 29
NTSB Railroad Accident Report
National Transportation Safety Board 30
the day of the accident was out of the ordinary for this individual. The results of that comparison
are shown in figure 10.
42
Records covering the 28 days before the accident showed 5 days with no text messaging
and 4 days with more than 100 text messages sent or received in a 24-hour period. Activity on
the remaining 19 days averaged about 40 messages per day.
The records also reflected the engineer’s use of a wireless device to make voice calls
while on duty. Figure 11 shows the telephone calls the engineer made or received (except for any
that may have gone to voice mail) on the day of the accident and the preceding 7 days.
The General Code of Operating Rules
43
addresses the use of wireless or other electronic
devices by train crewmembers as follows:
Rule 1.10 Games, Reading, or Electronic Devices
Unless permitted by the railroad, employees on duty must not:
• Play games.
• Read magazines, newspapers, or other literature not related to their duties.
• Use electronic devices not related to their duties.
Metrolink Timetable No. 5 Additions and revisions to General Code of Operating Rules
dated July 8, 2008, adds to Rule 1.10:
[Unless permitted by the railroad, employees on duty must not:]
• Use cellular telephones when operating the controls of moving equipment
except in emergencies.
Connex Metrolink Notice No. 17.08, on July 8, 2008, added the following to the previous
version of the notice:
Electronic Devices:
The inappropriate use of electronic devices by employees on duty has been shown
to be a contributing factor in personal injuries and rule violations. While you are
working you are obligated to be completely focused on your job and the safe
transportation of passengers. As a result, under most circumstances employees are
prohibited from having personal electronic devices turned on and/or in their
immediate vicinity while working.
42
The times of train operation shown on the graph were taken from the engineer’s time tickets, but these times
may differ somewhat from the actual times that the engineer was responsible for operating a train.
43
These rules apply equally to all railroads operating over SCRRA tracks.
NTSB Railroad Accident Report
National Transportation Safety Board 31
Here are some examples of when company or personal cellular phones must not
be used:
• While on the ground lining switches, meeting trains, standing next to main
tracks or when performing other duties that require your undivided
attention to safety and rules compliance
• While in the control compartment of a moving train
• To conduct non-railroad business while on or near trains
• Here are some examples of when company or personal cellular phones
may be used:
• While in a layover facility
• When communicating railroad business on a stopped train such as
troubleshooting mechanical problems or reporting information relating to
an incident as the incident commander
• When in a crew transportation van
• Conductors reporting information to dispatchers relating to delays, etc., as
long as the Conductor is not in the control compartment of a moving train
• Remember, when the train is moving or you are on the ground performing
railroad business your personal electronic devices must be turned off and
must not be within your reach-for example on the control stand or on your
person. Personal electronic devices may be carried in your grip[
44
] if they
are turned off. Conductors must have their company cellular phones “on”
at all times while on duty.
Metrolink conductors (who have overall responsibility for the train except for its
mechanical aspects and train handling) are issued a company cell phone to facilitate their
communication with dispatchers. Train 111’s conductor told investigators that he was allowed to
use the cell phone for company business when actually on board the train. On the day of the
accident, he used his company-provided cell phone to report the collision.
The Metrolink conductor said that about a month before the accident, in early August
2008, he observed the accident engineer using his cell phone while he (the engineer) was in the
control compartment of a train preparing to leave the Moorpark station. He said he spoke to the
engineer about it and the engineer, responding that he had been conducting union business,
acknowledged that he needed to put the device away. The conductor said he later brought the
incident to the attention of a supervisor but that he never heard back from the supervisor about
44
Grip refers to the bag of personal belongings most crewmembers carry to and from work assignments.
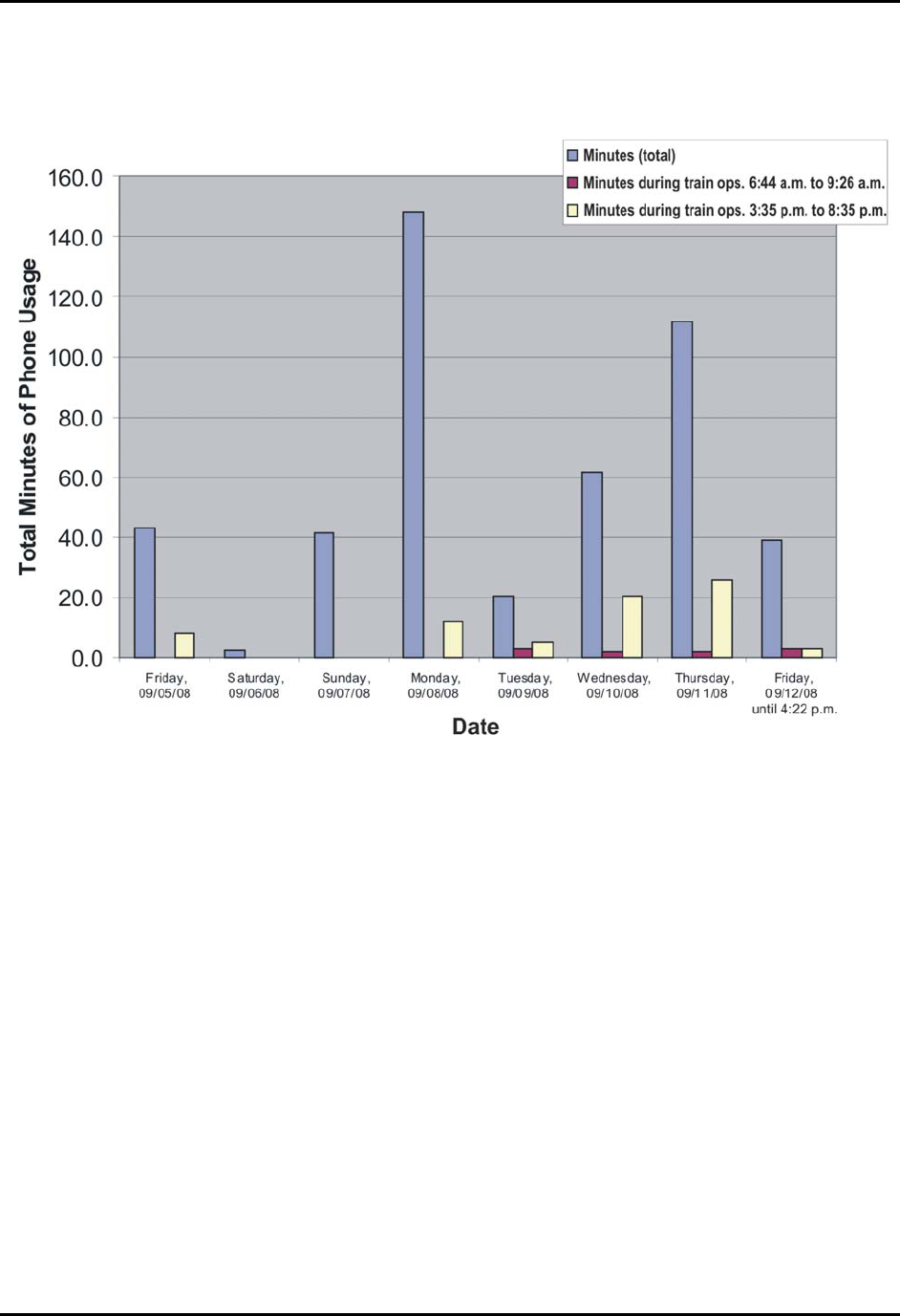
NTSB Railroad Accident Report
any action that had been taken with regard to the inappropriate cell phone use. He also said he
believed this to be an isolated event.
Figure 10. Text messages sent and received by the Metrolink engineer on the day of the
accident and on the previous 7 days. (The engineer did not work Saturday or Sunday.)
At the March 3 and 4, 2009, public hearing on this accident held at NTSB headquarters in
Washington, D.C., the Metrolink (Connex) manager of safety and operating practices recalled
that he was the one to whom the conductor had reported the engineer’s cell phone use. He said
he immediately followed up with the engineer, briefing him not only on General Code Rule 1.10,
but also on Connex’s cell phone policy:
During my conversation with him, I asked him where his phone was. He said it
was stored away in his grip, that it was off. We talked about the cell phone policy.
Confident that he understood the policy…, I did a couple observations within the
next 2 weeks, and that was the last of any conversations or observations with the
engineer [with regard to use of wireless devices].
National Transportation Safety Board 32
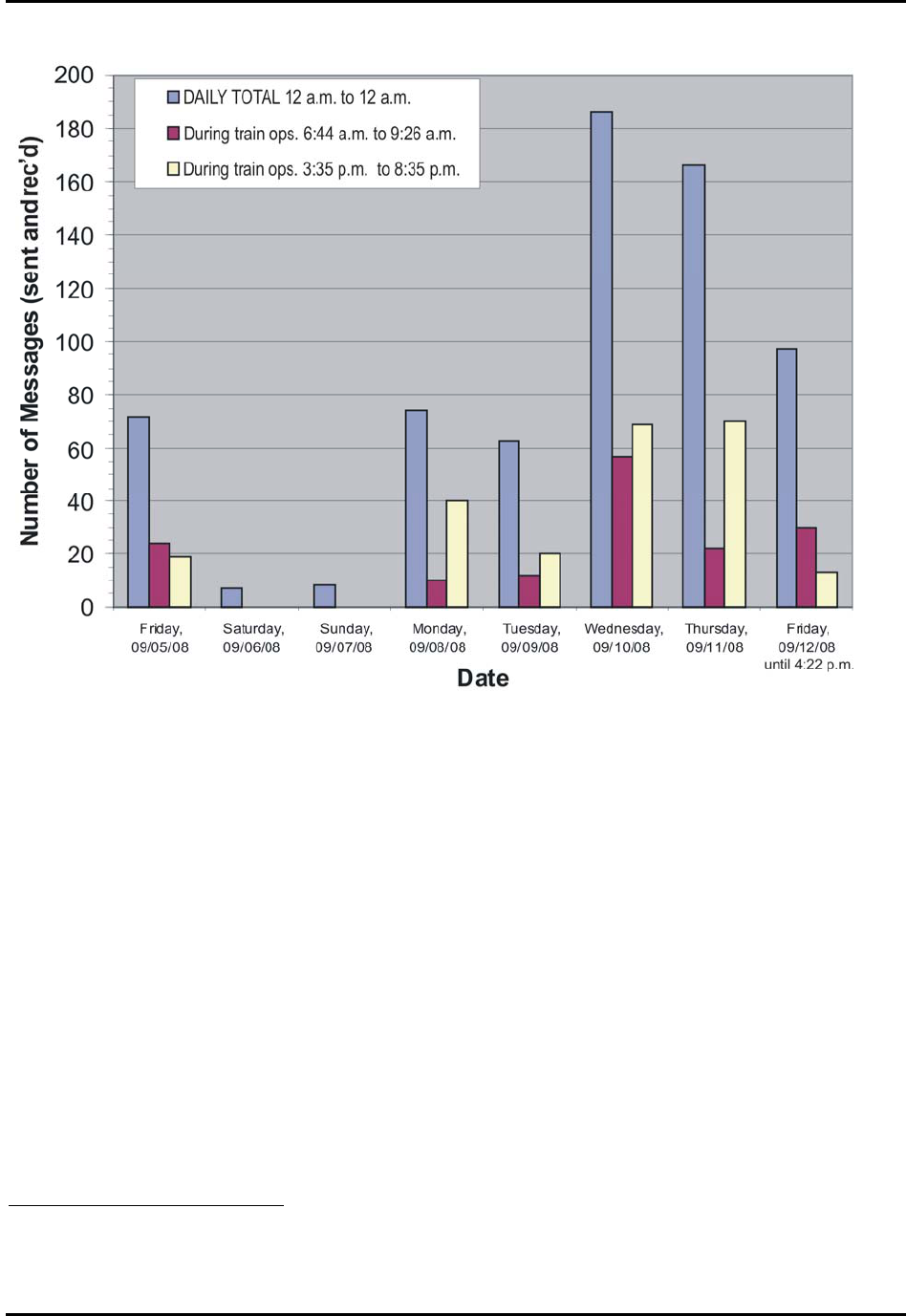
NTSB Railroad Accident Report
Figure 11. Telephone calls sent and received by Metrolink engineer on day of accident and on
previous 7 days.
Also at the public hearing, the safety and operating practices manager stated that on one
other occasion he had taken exception to the accident engineer’s use of a wireless device while
on duty. He said the incident occurred on September 7, 2006, shortly after the policy regarding
use of electronic devices by train crews had gone into effect. Several Metrolink, UP, and Amtrak
officers performed a joint “blitz” test in the Glendale and Burbank area to identify any possible
problems regarding the use of electronic devices and to remind employees of the policy. The
tests involved riding trains, stopping and boarding trains, and interviewing employees.
The manager stated that he boarded the engineer’s train at Burbank and arranged to have
another manager call the engineer’s cell phone.
45
The phone, which was in the engineer’s
briefcase, began ringing while the manager and engineer were conducting a job briefing in the
train’s operating compartment. The manager said he told the engineer that he was in violation of
the policy and that the violation would be entered into the company’s efficiency test reporting
45
According to testimony at the public hearing on this accident, Connex used this method of detecting
prohibited use of a wireless device until the issuance of Federal Emergency Order 26 (discussed later in this report)
on October 7, 2008.
National Transportation Safety Board 33

NTSB Railroad Accident Report
National Transportation Safety Board 34
system. He said the engineer told him that he was aware of the policy but that he had forgotten to
turn the device off when he had stowed it that morning.
Connex provided the NTSB with results of crewmember efficiency tests conducted since
June 25, 2005, that related to Rule 1.10. Of the 14 recorded observations, 10 resulted in citations
for noncompliance with the rule. Three observations involved a crewmember having a personal
cell phone turned on while operating the train. One of those was the aforementioned observation
involving the engineer in this accident.
The manager stated that, after the Chatsworth accident, Metrolink management had
become “very aggressive with inspecting for cell phones,” which included stopping and boarding
trains en route between stations rather than at station stops and closely inspecting trains and
crews. Asked if it was difficult to monitor use of a wireless device by an engineer alone in a
locked locomotive, he stated:
Oh, that's very difficult. …[A]s the train went by, you’d almost have to see a cell
phone up to their ear. You’d have to board the train undetected. We do board the
train en route from [a] station, but it is very difficult to get on a train. I’ll get on
the train, I'll have to unlock the door. Usually, the engineer will see you coming.
It’s extremely difficult to oversee.
Content of Text Messages
Verizon records for the 7 days prior to the day of the accident included the content of
most of the text messages sent and received by the Metrolink engineer. Most of the text
messages during the engineer’s morning trip on the day of the accident appear to be to and from
a coworker discussing some type of company correspondence. Six messages were to or from
Person A. All of the messages during the afternoon (accident) trip were to or from Person A.
These messages appear to be primarily discussing train schedules, how far behind schedule
certain trains are, and where different trains may or may not “meet” (pass one another) along the
track.
A review of the content of all of the engineer’s text messages over the previous 7 days
(including those during and outside the times the engineer was responsible for operating a train)
indicated that the engineer and Person A had been coordinating to allow Person A to operate
train 111 on the evening of the accident, starting at about 7:45 p.m. The intent was for Person A
to board the train at Moorpark and to operate it from Moorpark to Montalvo. A portion of one
exchange on September 8, 2008, (the Monday before the Friday accident) reads:
[Engineer to Person A ]: yea....but I’m REALLY looking forward to getting you in the
cab and showing you how to run a locomotive.
[Person A to Engineer]: Omg dude me too. Running a locomotive. Having all of that in
the palms of my hands. Its a great feeling. And ill do it so
good from all my practice on the simulator.
[Engineer to person A]: I’m gonna do all the radio talkin’...ur gonna run the locomotive
& I’m gonna tell u how to do it.
NTSB Railroad Accident Report
National Transportation Safety Board 35
Additionally, Person A and the engineer had arranged for a “ride-along” on the evening
of Tuesday, September 9. Person A and Person B were to board the engineer’s train at
Chatsworth and ride it to Union Station, which they apparently did. The text messages
concerning this “ride-along” were not as detailed as those outlining the plans to allow Person A
to operate the train; however, messages on the following day (September 10) indicate that Person
A was “up in the cab” and “touching the controls.” In the same context of the previous evening’s
activities, the engineer referred to “how much [Person C] wanted to stay in the seat.”
On the morning of September 10, the engineer sent to Person B a message that read:
“[Person B] you wanna run again tonight to montalvo??? if you can?” Later, another message to
Person B read: “this time I’m taking a picture of you @ da throttle!!!” A subsequent message
from the engineer to Person B read, “... we should have the 866 this evening...,” referencing the
locomotive unit number. Person B responded, “A bit tougher to get in and out of the cab but it
should be fine”.
A number of messages between Person A and the engineer on the day of the accident, as
well as on the days leading up to the accident, addressed concerns that the riders would be seen
either entering the locomotive or while occupying the cab. Apparently, on the afternoon of the
accident, the engineer e-mailed Person A with the plan for boarding the train at Moorpark, to
which Person A responded:
[Person A to Engineer]: Very crafty. Looks good man. And i will have my cell phone.
About 6 minutes later, Person A messaged:
[Person A to Engineer]: Ok got it printed out. Makes perfect sence [sic]. I think you’ll
be on the main.
Connex Metrolink Notice No. 17.08, dated July 8, 2008, states:
Head End Authorization:
Only the engineer of record, conductor of record, mechanical riders, operating
managers and others with proper written authorization are permitted on the head
end and/or control compartment of Metrolink trains.
The last message received by the engineer from Person A arrived at the engineer’s
wireless device at 4:20:57, about the time train 111 was accelerating out of Chatsworth station.
Content of that message was as follows: “I would like that too [referring to a possible meet with
other trains, the topic of a previous text message]. We already need to meet 796. That would be
best.” At 4:22:01, about 22 seconds before the collision, the Verizon network recorded that the
engineer had sent the following response to Person A: “yea…usually @ north camarillo.”
Leesdale Local Conductor’s Use of a Wireless Device
Information came to light after the accident to the effect that the Leesdale Local’s
conductor may have been using a wireless device during the time he was responsible for the
operation of his train. To follow up on this information, NTSB investigators obtained the

NTSB Railroad Accident Report
National Transportation Safety Board 36
Verizon Wireless records for the conductor’s account. These records include the time and date of
incoming and outgoing telephone calls, as well as the time and date of text messages sent and
received. The content of the text messages was not available because the date of the request for
the records was beyond Verizon’s standard retention period for those records.
The Leesdale Local’s conductor made three telephone calls while on duty on the day of
the accident. These calls appear to be business-related, as they were all to a telephone number
associated with the issuance of Metrolink track warrants (authorizations for a train to occupy a
certain segment of track for a certain period of time).
The records indicate that the conductor sent or received a total of 41 text messages while
on duty between 11:30 a.m. and 4:20 p.m. on the day of the accident. According to the
“Conductor’s Report,” the conductor was on a moving train between 12:29 p.m. and 1:55 p.m.,
and again from 3:13 p.m. until the accident at 4:22 p.m. During this time, the conductor sent or
received a total of 35 text messages. His last outgoing text message was received and logged by
the Verizon network at 4:20 p.m., about the time his train exited tunnel 26 and passed signal
4426.
At the public hearing on this accident, the UP general manager of operating practices
stated that the conductor’s efficiency test records covering the previous 12 months showed no
exceptions with regard to his use of electronic devices. At the time many of the text messages
were sent, including the last one transmitted about 2 minutes before the collision, the conductor
was occupying the locomotive cab along with the engineer. In postaccident interviews, the
engineer did not mention that the conductor had used such a device on the day of the accident.
Asked at the public hearing what action an employee should take in such a circumstance, the
general manager of operating practices stated:
A fellow crewmember should remind the employee of the rule requirement and
tell them they need to turn the cell phone off to be in compliance to the rule. We
would expect that of any manager onboard; we certainly would expect it between
two crewmembers.
Tests and Research
Sight-Distance Tests of Trains
For the sight-distance tests, exemplar locomotives simulating those of the Metrolink and
UP trains were positioned facing each other at the point of collision. The locomotives were then
moved away from each other in intervals of 60 feet (representing the approximate distance a 40-
mph train will travel in 1 second) until the engineer aboard each locomotive could not see the
other train. These tests revealed that each engineer’s first view of the opposing train would have
occurred when the trains were about 540 feet apart. At that point, at a closing speed of about 80
mph, the trains would have been 4 to 5 seconds from impact. (See figure 12.)
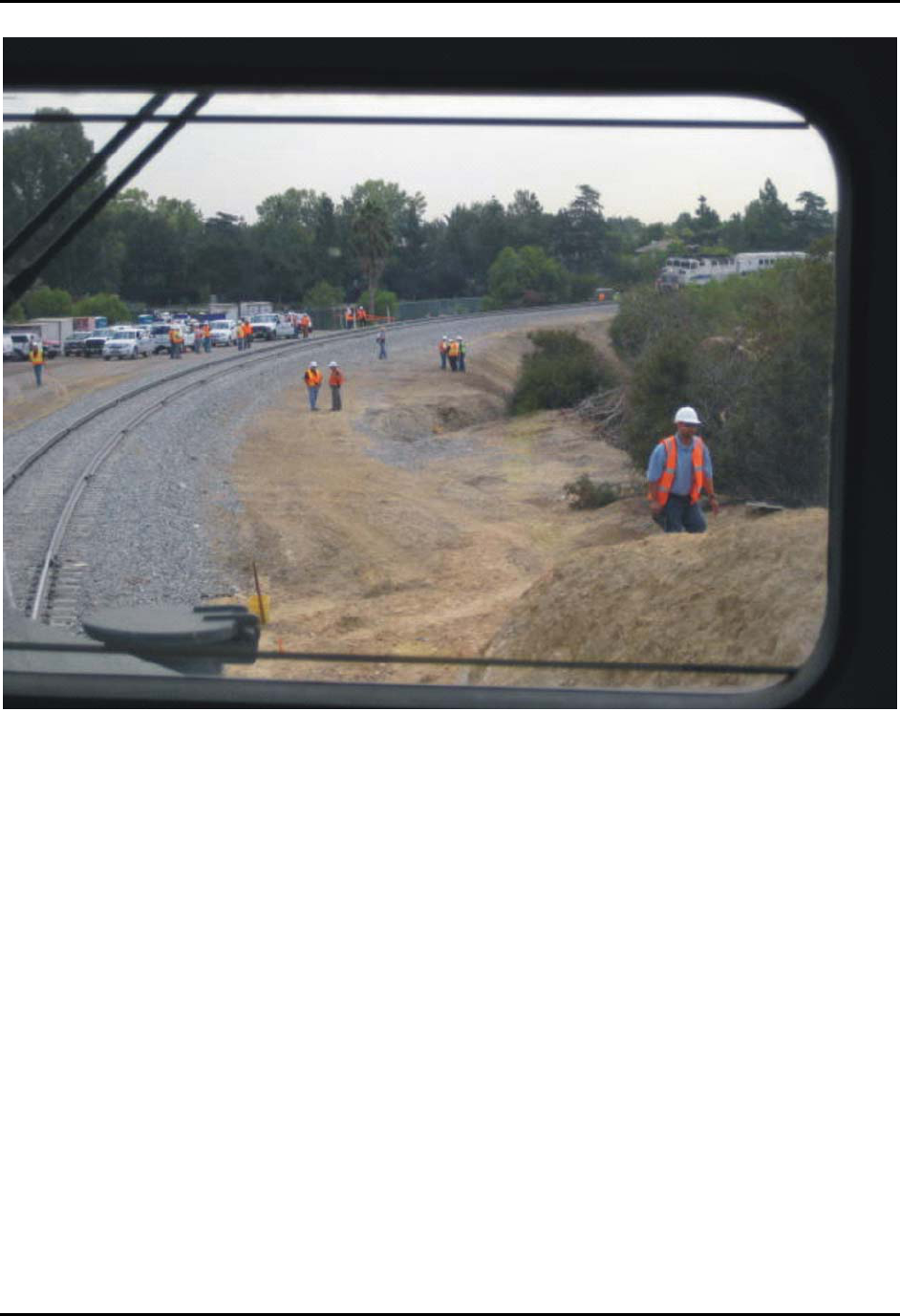
NTSB Railroad Accident Report
Figure 12. View from the head end of a simulated Leesdale Local during train sight-distance
testing. At a closing speed in excess of 80 mph, the trains would be only seconds from impact
as the Metrolink train becomes visible around the curve.
Sight-Distance Tests of Signals
Investigators also conducted sight-distance tests for the signals train 111 encountered
before arriving at Chatsworth station as well as for the signal display and switch point
configuration at CP Topanga.
Signal Aspects East of CP Topanga. For each test of the signals east of CP Topanga, a
Metrolink train consist was moved westbound (toward the signal) until the test engineer affirmed
that he had a clear view of the signal aspect. The tests confirmed that the aspect of signal 4483
(the westbound signal immediately before CP Bernson), could be seen and identified from 1,832
feet. The aspect of the westbound signal at CP Bernson could be seen and identified from 5,353
feet. Signal 4451 (the intermediate signal train 111 encountered before entering Chatsworth
station) could be seen and identified from 1,360 feet.
Signal Aspect at CP Topanga. The westbound signal at CP Topanga consists of a three-
aspect (green, yellow, red) signal head on a mast. Each aspect is 8 3/8 inches in diameter. The
centers of the yellow and green lenses are 21 feet 6 inches above the ground. The center of the
National Transportation Safety Board 37

NTSB Railroad Accident Report
National Transportation Safety Board 38
red lens is 20 feet 5 inches above the ground. The control compartment of a locomotive typically
positioned at the Chatsworth station is about 5,288 feet from the signal.
The conductor of train 111 told investigators that, just before the train departed
Chatsworth station, he could see the CP Topanga signal, and the signal aspect was green. Three
individuals—a station security guard and two rail fans—who were on the station platform at the
time (and who were on a first-name basis with both the engineer and conductor of train 111) also
stated that they had seen the Topanga signal displaying a green aspect after train 111 left the
station. One of the rail fans told investigators that the CP Topanga signal was not readily visible
from the Chatsworth station platform. He said the signal could be seen if one were to approach
the edge of the platform and “lean out,” and that this is what he had done as train 111 departed
the station on the day of the accident. One of the rail fans also told investigators that it had been
his experience at the Chatsworth station that it was not possible to see a red signal at CP Topanga
in the daytime, only at night.
On September 15, 2008, the NTSB conducted sight-distance tests of the signal to assess
overall visibility of the signal from the vantage point of the Metrolink train conductor and
engineer and to determine if ambient light conditions, reflections, or atmospheric conditions
could affect an observer’s interpretation of the signal aspects. These observations were carried
out at the same time of day as the accident.
For the tests, the Metrolink dispatcher aligned the CP Topanga switch for eastbound
movement into the siding (as it was on the day of the accident) so that the westbound signal at
CP Topanga would display a stop indication. About 4:20 p.m., investigators made unaided visual
observations of the signal from the conductor’s position on the platform as well as from the
platform adjacent to the point at which the train 111 locomotive would have been positioned.
Some observers reported seeing an intermittently visible “faint glimmer” of red; other observers
reported seeing nothing.
About 4:30 p.m., investigators boarded the cab of a three-car Metrolink train while it was
positioned at its typical spot alongside the Chatsworth station platform. The Metrolink engineer
who participated in the test stated that he could see the signal at Topanga, but he noted that he
knew where to look through experience.
The engineer was instructed to depart the station westbound as he normally would and to
stop at the point where he could clearly distinguish the red CP Topanga signal. The engineer
stopped short of the first road crossing (Devonshire Avenue) and said that he could clearly see
the signal. Some members of the observation group reported seeing the signal clearly, while
others reported still seeing only an intermittently visible flickering red. At this point the train had
traveled 953 feet from the station and was still 4,335 feet from the signal.
The train was then backed up and spotted normally at Chatsworth station. The Metrolink
dispatcher aligned CP Topanga for the train’s movement westbound in order to have the CP
Topanga signal display a green aspect (clear indication). At 4:45 p.m., the signal displayed a
flashing yellow aspect (advance approach indication) that was clearly visible to all observers
both in the locomotive cab and in the cab control car.
At 4:46 p.m., the CP Topanga signal displayed a green aspect that again was clearly
visible to all observers. At 4:51 p.m., the signal displayed a red aspect. The red signal was faint
NTSB Railroad Accident Report
National Transportation Safety Board 39
and only intermittently visible from both the locomotive cab and the conductor’s position in the
cab control car. Not all observers were able to see this signal aspect.
CP Topanga Switch Alignment. To test visibility of the position of the switch points at
the CP Topanga switch, investigators had an engineer back a Metrolink consist eastbound until
he could no longer see the position of the switch points. This distance was determined to be
about 615 feet.
Testing of Signal System
Postaccident inspection of the signal system found that all signal units and signal cases at
the intermediate signals and at the control points Topanga, Bernson, and Davis were locked and
sealed with no indications of tampering or vandalism to any of the signal equipment.
Investigators examining the signal head of the westbound CP Topanga signal found the signal
head to be clean internally with all electrical wiring and connections intact and in good overall
condition. The signal head was found to be sealed against external light sources.
Mechanical and electrical tests were performed on all switch and signal components at
CP Topanga. The tests confirmed that, except for components damaged as a result of the
accident, all switch and signal components worked as designed. Testing of the Vital Harmon
Logic Controller confirmed that conflicting routes could not be cleared simultaneously.
The Metrolink dispatch center aligned the route as it was at the time of the accident,
46
and investigators used rolling shunts
47
to simulate the movements of Metrolink train 111 and the
Leesdale Local. Signal personnel positioned at CP Davis, at intermediate signal 4426; at the east-
and westbound signals at CP Topanga, at intermediate signal 4451, and at CP Bernson confirmed
that the signal system functioned as designed and intended.
While the route was aligned for an eastbound train movement into the siding at CP
Topanga, investigators, as a test, sent a request for the westbound Topanga signal to clear. The
Harmon Vital Logic Controller at that location would not act on this command, and the
westbound signal did not clear. The controller is designed to ensure that lamp output energy is in
compliance with the requested signal aspect and that an internal or external fault will not result in
an improperly displayed signal. With the eastbound signal at Topanga displaying clear,
investigators applied battery power to the green signal lamp of the westbound signal. Within 1
second, the Harmon Vital Logic Controller detected the improperly illuminated lamp and, as
designed, changed the eastbound Topanga signal from clear to stop and started a 6-minute timer,
which effectively locked out the control point and prevented any commands from being acted
upon.
46
On the day of the accident, the dispatcher had stacked the route for the westbound movement; on the day of
the testing, the westbound route requests were not stacked.
47
Shunting the track refers to connecting the two rails electrically to simulate the presence of a train. With a
rolling shunt, shunts are installed then repositioned in a pattern that simulates a train’s movement along a block of
track.

NTSB Railroad Accident Report
National Transportation Safety Board 40
As an additional test, investigators had the CP Topanga switch aligned for eastbound
movement into the siding and locked. They then initiated a request to clear the Topanga
westbound signal. This test was performed once with the eastbound signal displaying clear and
again with the signal displaying stop. The logic controller would not act on either command and
did not clear the westbound signal.
The validity of the downloaded signal event recorder data was confirmed by a review of
recordings from the forward-looking video camera of the Leesdale Local, which showed that all
signals encountered by the Local were displaying their proper aspects as indicated by the signal
recorder data.
Examination of the Metrolink signal data log and signal maintenance records did not
identify any condition that would have prevented the signal system from operating as designed.
Signal trouble reports for the 6 months preceding the accident were reviewed, and no exceptions
were noted for the westbound signal at CP Topanga.
Testing of Communications System
On September 17, 2008, three communications tests were conducted to determine
whether communication “dead spots” existed along the route of Metrolink train 111 that would
have interfered with radio transmissions between train crewmembers or that would have
prevented radio transmissions from being recorded by the dispatch center. All the tests were
conducted using handheld radios, including the radio that was in the possession of the train 111
conductor on the day of the accident.
48
The first test involved making radio transmissions every 2 minutes from on board an
exemplar train as it traveled eastbound from the Simi Valley station to the Northridge station.
The second test was the same as the first except that the train was traveling westbound from
Northridge to Simi Valley. The dispatch center confirmed that the communications were
successful, with the only exception being a loss of communication inside tunnel 26.
The final test was done on the ground east and west of CP Topanga. The test was
distance-based and was designed to evaluate communication between the handheld radio and the
dispatch center. The only failed communications noted were within 100 feet of the portal of
tunnel 28.
The handheld radio being used by the conductor of Metrolink train 111 on the day of the
accident was determined to be fully functional. Testing of the handset battery revealed that when
fully charged, the battery lost capacity over a relatively short period of time, which reduced the
radio’s transmit power. Testing showed that after three to five talk cycles, the audible low-
battery warning activated at the end of each subsequent talk cycle.
48
The in-cab radio the train 111 engineer used for all his radio transmissions on the day of the accident was
destroyed in the accident and was therefore not available for testing.
NTSB Railroad Accident Report
National Transportation Safety Board 41
Inspection and Testing of Track
Investigators made postaccident inspections of the track geometry west of CP Topanga
and took measurements at a total of 25 stations in the undisturbed track to the east of the point of
collision. (No measurements were taken to the west of the point of collision because of
disturbances to the track as a result of the accident and the subsequent repair work.) The
measurements revealed track conditions as follows:
Track Gage. Widest gage (distance between the inside faces of the running rails) was
measured at 56 7/8 inches. FRA Track Safety Standards permit a maximum gage of 57 3/4
inches in class 3 track.
Track Alignment. The maximum alignment (relative positions of the two rails laterally)
deviation in undisturbed track measured 5/16 inch. FRA Track Safety Standards permit a
maximum deviation of 1 3/4 inch in class 3 track.
Cross Level. Greatest deviation in cross level (difference from the specified elevation
between the two rails) was measured as 5/16 inch. FRA Track Safety Standards permit a
maximum deviation of 1 11/16 inch in class 3 track.
Overall, no unacceptable conditions were found in the geometry of the track.
Other Information
Postaccident Actions by SCRRA
According to SCRRA representatives, after the accident, SCRRA put into place a
Metrolink Enhanced Safety Action Plan that incorporates the following elements:
Safety Culture
• Elevated the Safety Department to report directly to the SCRRA chief executive
officer (CEO), with safety manager required to meet with CEO at least weekly, to
provide CEO with monthly written updates, and to provide the SCRRA board with
quarterly updates.
• Created a Strategic Safety Leadership Team comprising all operating general
managers, SCRRA contract managers, and the CEO. The leadership team:
• Meets quarterly with the goal of sharing information on common problems, on
best practices, and on future safety efforts by SCRRA.
• Reviews safety performance by SCRRA and its contactors
• Established a risk-assessment process.
• Is developing goals with regard to training, efficiency testing, rules violations,
injuries, audits/inspections.

NTSB Railroad Accident Report
National Transportation Safety Board 42
SCRRA Organizational Structure
• Hired an assistant director of equipment.
• Hired a manager of field operations and three operations compliance officers.
• Established a new field operation unit responsible for efficiency testing of foreign line
trains operating over SCRRA territory as well as performing oversight testing of the
SCRRA contract operator.
• Created a System Safety Committee structure that involves all organizational layers,
including contractors.
Metrolink Operations
• Updated the Metrolink operational testing program.
• Hired an operating rules manager responsible for implementing the updated
efficiency testing program.
• Increased observations of engineers, conductors, and other safety-critical employees
as well as increased joint testing with other operators on the territory.
• Installed inward- and forward-facing cameras on its locomotives to monitor engineers
for compliance with rules regarding electronic devices, unauthorized personnel in the
operating compartment, and sleeping, and has established a program for the routine
reviewing of the recorded images.
49
Metrolink Safety Projects
• Accelerating the development and deployment of positive train control on the
Metrolink locomotive fleet by December 2012 and the installation of positive train
control on SCRRA territory by 2015.
• Has reassigned staff and hired 40 additional contract employees to oversee the
installation of positive train control, which includes a new dispatch system,
installation of the back office servers (BOS), retrofitting of the locomotive and
cab car fleet for the new micro-processors and new video screens, training and
hiring of additional staff to support positive train control, re-spacing of
signals, and the development of algorithms for stopping distances of
commuter equipment.
• Is working with the FRA and the railroad industry on communication,
equipment and operating rules in advance of the December 2012 commitment.
49
The Brotherhood of Locomotive Engineers and Trainmen has filed suit in U.S. District Court to prohibit
SCRRA from using its in-cab audio and video system for this purpose.

NTSB Railroad Accident Report
National Transportation Safety Board 43
• Has installed 43 additional Inert Inductor Automatic Train Stop systems to alert
engineers to the need to reduce speed. The inert inductors require that the engineer
acknowledge a reduced speed requirement of 20 mph or more within 8 seconds or
receive a penalty brake application.
• Is purchasing Crash Energy Management cab control cars and trailer cars that will be
placed in operation starting in 2010. These cars will have crash-energy seats,
frangible tables, and push-back couplers. The existing fleet will be retrofitted with
crash energy seats, push-back couplers, and frangible tables.
• Is installing new LED lights at all control point signals, to be completed in 2010.
Federal Rules Regarding Wireless Devices
In its investigation of a May 28, 2002, collision of two Burlington Northern Santa Fe
freight trains near Clarendon, Texas,
50
the NTSB determined the probable cause of the accident
to be, in part, “the coal train engineer’s use of a cell phone during the time he should have been
attending to the requirements of the track warrant for his train.” As a result of that investigation,
the NTSB made the following safety recommendation to the FRA:
R-03-1
Promulgate new or amended regulations that will control the use of cellular
telephones and similar wireless communication devices by railroad operating
employees while on duty so that such use does not affect operational safety.
In its October 2003 response to this recommendation, the FRA stated its belief that the
railroad industry’s establishment and enforcement of its own operating rules governing cell
phone use were sufficient to address the issue without the need for Federal action. The FRA also
noted that it would continue to “closely monitor railroad compliance with their operating rules
restricting cell phone use and will not hesitate to take appropriate enforcement action if it
becomes necessary.”
During a March 2004 meeting with NTSB staff, FRA representatives indicated that the
agency had issued instructions to FRA staff to be mindful of their own use of cell phones, but
they suggested that enforcing a Federal rule would be almost impossible. The FRA did, however,
refer the issue to its Railroad Safety Advisory Committee for discussion as to whether the issue
should be addressed by a new safety advisory committee working group. Based on this response,
Safety Recommendation R-03-1 was initially classified “Open—Acceptable Response.”
When the issue of a new or amended Federal regulation was subsequently brought before
the Railroad Safety Advisory Committee, the members agreed that the complexity of the issue
was such that the committee was not prepared at that time to consider a Federal rule. On March
7, 2007, the NTSB, noting that little progress had been made in almost 3 1/2 years from the date
50
Collision of Two Burlington Northern Santa Fe Freight Trains Near Clarendon, Texas May 28, 2002,
Railroad Accident Report NTSB/RAR-03/01 (Washington, DC: National Transportation Safety Board, 2003).
NTSB Railroad Accident Report
National Transportation Safety Board 44
the recommendation was issued, reclassified Safety Recommendation R-03-1 “Open—
Unacceptable Response.” Thus, at the time of the accident, no Federal rail regulations prohibited
the use of cell phones or similar devices by train crewmembers.
On October 7, 2008, after and in response to the Chatsworth accident, the FRA issued
Emergency Order 26, Emergency Order To Restrict On-Duty Railroad Operating Employees’
Use of Cellular Telephones and Other Distracting Electronic and Electrical Devices,
51
which
details the circumstances under which train crewmembers could use both company-supplied and
personal electronic devices.
With regard to personal electronic devices, Emergency Order 26 states:
(c) Personal electronic and electrical devices. (1) Each personal electronic or
electrical device must be turned off with any earpieces removed from the ear
while on a moving train, except that, when radio failure occurs, a wireless
communication device may be used in accordance with railroad rules and
instructions.
(2) Each personal electronic or electrical device must be turned off with any
earpieces removed from the ear when a duty requires any railroad operating
employee to be on the ground or to ride rolling equipment during a switching
operation and during any period when another employee of the railroad is
assisting in preparation of the train (e.g., during an air brake test).
(3) Use of a personal electronic or electrical device to perform any function other
than voice communication while on duty is prohibited. In no instance may a
personal electronic or electrical device interfere with the railroad operating
employee’s performance of safety-related duties.
Because Emergency Order 26 met the intent of Safety Recommendation R-03-1, the
NTSB, on September 17, 2009, reclassified recommendation R-03-1 “Closed—Acceptable
Alternate Action” At the same time, the NTSB expressed its disappointment that the FRA had
not taken previous action on this important safety recommendation.
FRA Emergency Order 20 (1996)
On February 20, 1996, in the wake of fatal collisions involving commuter trains near
Secaucus, New Jersey,
52
and Silver Spring, Maryland,
53
the FRA issued Emergency Order 20,
Notice No. 1, Emergency Order Requiring Enhanced Operating Rules and Plans for Ensuring
51
Federal Register, vol. 73, no. 195 (October 7, 2008), p. 58702.
52
Near Head-On Collision and Derailment of Two New Jersey Transit Trains Near Secaucus, New Jersey,
February 9, 1996, Railroad Accident Report NTSB/RAR-97/01 (Washington, DC: National Transportation Safety
Board, 1997).
53
Collision and Derailment of Maryland Rail Commuter MARC Train 286 and National Railroad Passenger
Corporation Amtrak Train 29 Near Silver Spring, Maryland, on February 16, 1996, Railroad Accident Report
NTSB/RAR-97/02 (Washington, DC: National Transportation Safety Board, 1997).

NTSB Railroad Accident Report
National Transportation Safety Board 45
the Safety of Passengers Occupying the Leading Car of a Train. The emergency order imposed
rule enhancements involving compliance with signal indications and addressed issues related to
passenger safety and emergency egress. As refined by Emergency Order 20, Notice No. 2, issued
on March 5, 1996, the order required that commuter and intercity passenger railroads issue an
operating rule as follows:
(A) If a passenger train operating in the block immediately preceding an
interlocking or controlled point stops for any reason, [including a station stop] or
its speed is reduced below 10 m.p.h., the train shall proceed under the reduced
speed set forth in applicable operating rules governing such circumstances and be
prepared to stop before passing the next signal. In no event shall this reduced
speed exceed 40 m.p.h., although lower speeds are permissible. The train must
maintain the prescribed reduced speed until the next wayside signal is clearly
visible and that signal displays a proceed indication.
The order further required that:
(E) Within 30 days of issuance of the railroad's rule, an appropriate qualifying
appurtenance shall be affixed to each signal governing the approach to an
interlocking or controlled point signal to serve as a visual reminder to the
engineer. Appropriate signage shall be displayed at the departure end of passenger
stations located in the block immediately preceding interlockings or controlled
points.
At the time the FRA issued Emergency Order 20, Metrolink operating rules included the
following:
9.9: Train Delayed Within a Block
If a train has entered a block on a proceed indication that does not require
restricted speed, and the train stops or its speed is reduced below 10 MPH, the
train must:
…B. CTC or Manual Interlocking Limits
Proceed prepared to stop at the next signal until the next signal is visible and that
signal displays a proceed indication.
Passenger trains operating in push/pull service must not exceed 40 MPH until the
next signal is visible and that signal displays a proceed indication.
Based on Operating Rule 9.9, Metrolink petitioned the FRA for relief from the signage
requirement of the emergency order. On April 30, 1996, the FRA granted Metrolink the waiver:
conditioned on the fact that the current operating rules require compliance with
the delayed-in-block rule by all trains, in all blocks, at all times. Under these
circumstances, FRA agrees that the placement of signage required by EO 20
could send a mixed and confusing message to operating crews concerning the
application of the rule.

NTSB Railroad Accident Report
National Transportation Safety Board 46
Analysis
Exclusions
Based on UP and Connex records, the crewmembers of both the Metrolink and UP trains
were experienced railroaders fully qualified to perform their duties. Examination of the work/rest
histories of all crewmembers did not indicate that any crewmember was experiencing fatigue that
would have affected performance before or at the time of the accident. The engineer and
brakeman on the Leesdale Local were on their regular assignment and, for several days before
the accident, had gone on duty at 11:30 a.m. and off duty at 6:30 or 7:00 p.m., thus experiencing
consistent work/rest patterns to which they were accustomed. The train’s conductor was an extra
employee filling in for the regularly assigned conductor. He had worked the Leesdale Local on
Monday before the accident and had been off Tuesday, Wednesday, and Thursday before being
called to work the Leesdale Local again on Friday. He had maintained a fairly consistent
wake/rest cycle during his days off.
The Metrolink train 111 engineer had also maintained the same work schedule for the 4
days leading up to the accident, going on duty at 5:54 a.m. and working until 9:26 a.m., then
returning for the second part of his shift at 2:00 p.m. and working until 9:05 p.m. On the day of
the accident, according to the conductor on the Metrolink train, the engineer said he had taken a
nap during his mid-day break and was well rested when he reported for work for his afternoon
tour of duty.
Based on the operator’s height and weight at the time of his last physical examination, he
had a calculated body mass index (BMI) of 34.4. By this calculation, the operator would have
been considered obese (a BMI greater than 30 constitutes obesity). Obesity is significantly
associated with an increased risk for obstructive sleep apnea (OSA), which can result in fatigue
and significant cognitive and psychomotor deficits. In addition, the engineer had previously
noted possible snoring and was noted on autopsy to have enlargement of the chambers of his
heart. Right-sided heart chamber enlargement, in particular, has been associated with severe
sleep-disordered breathing (including OSA).
54
However, the engineer had not been evaluated for
or diagnosed with sleep apnea, and he remained actively engaged in operating his train during his
afternoon shift, including making regular station stops and calling out some, though not all, of
the signals the train encountered along its route. During the approximately 2 minutes that elapsed
between the time train 111 departed Chatsworth station until the accident, the engineer was
engaged in text messaging, manipulating the throttle, sounding the train horn and bell, and
making brake adjustments, with no period of inactivity that might have suggested a lack of
alertness due to fatigue or lack of sleep.
54
U. C. Guidry, L. A. Mendes, J. C. Evans, D. Levy, G. T. O’Connor, M. G. Larson, D. J. Gottlieb, E. J.
Benjamin. “Echocardiographic Features of the Right Heart in Sleep-Disordered Breathing: The Framingham Heart
Study,” American Journal of Respiratory and Critical Care Medicine. 164(6) September 15(2001):933-8.
NTSB Railroad Accident Report
National Transportation Safety Board 47
The engineer had a history of diabetes and high blood pressure and had been taking
prescription medications for these conditions. He had also tested HIV positive and was being
treated with anti-retroviral medications. According to his medical records, his conditions were
under good control, and no adverse side effects were reported from his medication use.
Information downloaded from event recorders aboard the locomotives of the Leesdale
Local indicated that the train had been operated in accordance with signal indications from the
time it entered the main track at CP Davis until the accident. Correlation between event recorder
and sight-distance data indicate that emergency braking was applied 1 to 2 seconds after
Metrolink train 111 came into view, but the time and distance were insufficient for the braking to
have prevented or reduced the severity of the accident.
Postaccident toxicological tests were conducted on each crewmember of the Leesdale
Local, as well as the conductor of the Metrolink train 111. Specimens were also obtained from
the engineer of train 111. Except for those of the UP conductor, all specimens were negative for
the presence of alcohol as well as for FRA-specified illicit drugs.
The UP conductor tested negative for alcohol but was positive for marijuana in both his
blood and urine. The relative amounts of tetrahydrocannabinol (the active substance in
marijuana) and its metabolite suggest use within about 12 to 20 hours of the blood being
drawn.
55
Based on the reported times the blood and urine specimens were taken, the conductor
likely used marijuana within 3 to 11 hours of the accident. If so, it is possible that he was
impaired at the time of the accident.
56
However, the Leesdale Local was being operated in
compliance with signal indications on its approach to the siding at Chatsworth; thus the
conductor’s marijuana use was not a factor in the accident.
After the accident, the cars of both trains that had not been destroyed in the accident were
inspected and tested. Air brake and mechanical tests confirmed that the equipment was in good
working order, with no anomalies noted that would have contributed to the accident. Similarly,
the track segment train 111 traversed in the moments before the accident was found to be in good
condition, with all track geometry measurements falling within Federal tolerances for that class
of track.
It was daylight at the time of the accident. The weather was warm with clear skies and
calm winds. Although some haze was present, visibility was reported as 4 miles. Thus, no
meteorological conditions existed that would have impaired the train crews’ vision with regard to
signal aspects or that would have otherwise affected train operations.
55
Based on data in M. A. Huestis, J. E. Henningfield, E. J. Cone. “Blood Cannabinoids. II. Models for the
Prediction of Time of Marijuana Exposure from Plasma Concentrations of Delta 9-Tetrahydrocannabinol (THC) and
11-Nor-9-Carboxy-Delta 9-Tetrahydrocannabinol (THCCOOH),” Journal of Analytical Toxicology. 16(5) Sep-Oct
(1992):283-90.
56
See (a) R. C. Baselt. Drug Effects on Psychomotor Performance (Foster City, California: Biomedical
Publications, 2001). (b) V. O. Leirer, J. A. Yesavage, D. G. Morrow. “Marijuana Carry-Over Effects on Aircraft
Pilot Performance,” Aviation, Space, and Environmental Medicine. 62(3) March (1991):221-7. (c) J. A. Yesavage,
V. O. Leirer, M. Denari, L. E. Hollister. “Carry-Over Effects of Marijuana Intoxication on Aircraft Pilot
Performance: A Preliminary Report,” American Journal of Psychiatry. 142(11) Nov (1985): 1325-9.

NTSB Railroad Accident Report
National Transportation Safety Board 48
The NTSB therefore concludes that the following were neither causal nor contributory to
this accident: weather, fatigue, the engineer’s medical conditions or treatments, training and
experience of crewmembers, operation of UP Leesdale Local, alcohol or illegal drug use by
operating crewmembers, and condition of the track or rolling stock. The NTSB further concludes
that although the conductor of the UP Leesdale Local had likely used marijuana within 3 to 11
hours of the accident, this was neither causal nor contributory to the accident.
The Accident
On the afternoon of September 12, 2008, the Leesdale Local had completed its work and
was headed eastbound to its home terminal at Gemco. At the same time, Metrolink train 111 was
on its scheduled westbound run from Los Angeles Union Station to Montalvo. The two trains
would be using the same track, meaning that at some point one of the trains would have to divert
into a siding track and wait for the other to pass before it could continue its trip. Deciding when,
where, and how opposing trains will meet is the job of the dispatcher.
In this case, the dispatcher decided to allow the eastbound Leesdale Local to enter the
main track at CP Davis while westbound train 111 was still east of CP Topanga on the same
track. The dispatcher planned to have the freight train proceed to CP Topanga where it would
divert from the main track through the siding at Chatsworth. As soon as this move was complete,
train 111 would be able to continue westbound.
At 4:07:37 p.m., according to signal data logs, the switch at CP Topanga responded to the
dispatcher’s request and “reversed,” that is, aligned to force any eastbound train to move onto the
siding track rather than continue on the main track. The switch was now aligned against a
westbound train movement on the main track. The switch and signal circuitry for the controlling
westbound CP Topanga signal was designed such that, with the switch reversed, the westbound
signal could display no aspect other than red, or stop, for westbound trains.
With this first route programmed in, the dispatcher “stacked” the next route commands in
the sequence, requesting that the CP Topanga switch realign for the main track and that the
westbound signal clear for a westbound train movement after the freight train was fully in the
siding.
The signal system is designed such that a red aspect at westbound CP Topanga causes the
westbound signal at CP Bernson to display a flashing yellow aspect (advance approach
indication) and intermediate signal 4451 just east of Chatsworth station to display solid yellow
(approach indication) to approaching trains. Train 111’s engineer was recorded calling out the
flashing yellow signal at CP Bernson. He was not recorded calling out intermediate signal 4451
or the next signal, CP Topanga.
As train 111 departed Chatsworth station, the engineer proceeded as though the signal at
CP Topanga were green (clear) even though the flashing yellow at CP Bernson (which he
definitely saw and called) and the solid yellow at intermediate signal 4451 indicated that, at the
time train 111 passed them, the CP Topanga signal was displaying a red aspect. Even if
intermediate signal 4451 had been green, indicating that the signal at CP Topanga was, at that
time, also green, Metrolink’s delay-in-block rule would have required that the engineer leave

NTSB Railroad Accident Report
National Transportation Safety Board 49
Chatsworth station and proceed at no more than 40 mph until he could confirm the indication at
CP Topanga. Instead, the engineer accelerated his train to 54 mph.
About 2 minutes after leaving Chatsworth station, train 111 ran through and damaged the
CP Topanga switch, which had been aligned against westbound travel. At the time his train ran
through the switch, the engineer was not able to see the Leesdale Local advancing toward him.
His first possible view of the freight train would have occurred as his train entered the left-hand
curve just west of the switch. According to the locomotive data recorder, the engineer did not
apply the train brakes before impact. The Leesdale Local crew did promptly apply brakes on
their train when train 111 came into their view, but it was not possible to significantly slow the
train in the seconds that elapsed before the collision.
Emergency Response
Emergency responders arrived at the scene of the accident shortly after the initial
notification, and a unified command system was established with the responding agencies and
the railroads. Mutual aid resources were also requested from surrounding areas. During the
course of the response, the incident commander established a fire suppression group, an
extrication group, a medical group, a hazardous materials group, and an urban search and rescue
group. Firefighters, police officers, sheriff’s deputies, and highway patrol officers worked to
rescue, triage, and transport injured passengers and train crew. About 1,000 emergency personnel
responded.
As a result of the collision, the rear end of the locomotive telescoped into about two-
thirds of the first passenger coach, causing a complete loss of survivable occupant space.
Because of this damage, the extrication of passengers from the first coach was a difficult and
dangerous operation that required extensive manpower, resources, and time. Despite the
difficulties, responders carried out their duties as quickly and as efficiently as could be expected.
The NTSB therefore concludes that, considering the challenges of the recovery operations, the
emergency response to the accident was timely, well coordinated, and effectively managed.
As a result of the collision, fuel spilled from the Metrolink locomotive, and a fire burned
near the locomotives. During the firefighters’ fire suppression operations, they discovered that
two crewmembers were trapped inside the cab of the lead locomotive on the Leesdale Local. The
cab was filled with smoke. Firefighters eventually forced entry into the cab through a window
and rescued the crew, both of whom had suffered serious injuries. The NTSB concludes that
because locomotive cab exits are not designed to be quickly opened in an emergency, firefighters
could not rapidly enter the cab of the Leesdale Local to rescue the injured crew.
The NTSB addressed this issue during its investigation of a November 30, 2007, collision
of an Amtrak passenger train and a Norfolk Southern Railway Company freight train near
Chicago, Illinois.
57
In that collision, the forward portion of the Amtrak locomotive came to rest
57
Collision of Amtrak Passenger Train 371 and Norfolk Southern Railway Company Freight Train 23M
Chicago, Illinois, November 30, 2007, Railroad Accident Report NTSB/RAR-09/01 (Washington, DC: National
Transportation Safety Board, 2009).
NTSB Railroad Accident Report
National Transportation Safety Board 50
on top of a container on the rear car of the freight train. Because of structural damage to the
locomotive cab, the two engineers could not exit without assistance. As a result of the accident,
the NTSB made the following recommendation to the FRA:
R-09-3
Require that emergency exits on new and remanufactured locomotive cabs
provide for rapid egress by cab occupants and rapid entry by emergency
responders.
The FRA responded in May 2009 that it shares the NTSB’s concern about rapid egress
and rescue access for locomotive cabs, a concern that had been addressed, in part, through
previously issued regulatory design requirements for new locomotives. The FRA has also funded
new research into locomotive egress and rescue, to include concepts for a roof-mounted escape
hatch and an easily removable windshield system. The FRA further responded that it had
developed and provided to local emergency responders a training video titled “Locomotive
Emergency Response Operations.” Finally, the FRA stated that it would present this
recommendation and its actions to date to the Railroad Safety Advisory Committee’s
Locomotive Standards Working Group for further consideration. Based on this response, the
NTSB has classified Safety Recommendation R-09-3 “Open—Acceptable Response.”
Signals and Train Control
Signal Aspect at CP Topanga
In postaccident interviews, the train 111 conductor and three other individuals (two rail
fans and a security guard) who were on the Chatsworth station platform while the train served
the station stated that they had seen the CP Topanga signal as train 111 pulled out of the station
and that the signal was displaying a green aspect. Had this signal been displaying green, the
engineer’s actions after the train departed the station would have been appropriate, at least until
he was close enough to the CP Topanga switch to see that the switch was aligned against his
train. Had he realized that he was about to run through the switch, he would doubtless have taken
action to stop his train even if the signal had been green. But he took no action in his approach to
the switch, while running through it, or immediately afterward.
The evidence is incontrovertible that the CP Topanga switch was aligned for an
eastbound movement into the siding as westbound train 111 approached and went through it. The
damage to the switch points that was found after the accident could only have occurred as a
result of a run-through from the westbound direction. If this damage had occurred before the
arrival of train 111, the malfunctioning switch would have been detected by the computerized
dispatching system and would have shown on the dispatcher’s display as being “out of
correspondence,” a condition that would have caused all the CP Topanga signals to display red.
Once the switch is reversed and the switch points move away by a fraction of an inch
from the main track stock rail, the electrical path that would permit the westbound signal to
display a green aspect is interrupted, and the system does not allow the westbound signal at CP
Topanga to show any aspect other than red. In postaccident signal tests, investigators used an

NTSB Railroad Accident Report
National Transportation Safety Board 51
independent power source to illuminate the green lamp in the westbound CP Topanga signal
while the eastbound signal was showing clear (a green aspect), an action that would have placed
the two signals in conflict. Within 1 second, the logic circuits in the signal controller detected the
contradiction and responded by changing the eastbound signal from clear to stop and temporarily
locking the signals so that no commands could be acted upon. Even had some unknown anomaly
existed that would have permitted the westbound signal to display a green aspect while the
switch was reversed, that display would have been recorded on the signal data logs. Instead, the
data logs showed that the only signal repeater relay that was energized from the time the switch
was reversed until the time of the accident was the relay for the red lamp. The fact that this relay
was energized also shows conclusively that the red lamp was actually illuminated, because the
current needed to energize this relay must pass through the lamp. If the lamp bulb were missing
or burned out, this relay could not have been energized.
Inspection and testing of the lights themselves determined that the signal lamps and
lenses were undamaged and operating properly. Signal inspection records indicated no
deficiencies that would have prevented proper operation of the signal system. Finally, tests and
analysis of the signal event recorders, along with the Metrolink Control Center’s Digicon signal
event log, determined that the signal aspects were properly displayed and were not in conflict at
the time of the accident.
The NTSB therefore concludes that physical evidence, documentary and recorded data,
and postaccident signal examination and testing confirm that the westbound signal at CP
Topanga was displaying a red aspect at the time Metrolink train 111 departed Chatsworth station
and as it approached and passed CP Topanga, and had the engineer complied with this signal
indication, the accident would not have occurred.
Stacking of Routes
At the time of the accident, the dispatcher had “stacked” the routes for the Leesdale Local
and train 111. Even before the Leesdale Local had completed its planned move, the dispatcher
had entered commands to realign the CP Topanga switch and to change the westbound signal to
green. But these commands could only be carried out after the previous route had been
completed, that is, after the Leesdale Local was in the siding. The investigation determined that
the commands to realign the switch and clear the signal were still in the dispatching queue and
were never sent to the logic controllers in the field. Had these stacked commands been sent
prematurely, the logic controllers would have responded as they did during postaccident testing;
that is, they would have sensed a potential routing conflict and changed all the control point
signals to red until the conflict could be resolved. The NTSB therefore concludes that the signal
and traffic control systems worked as designed on the day of the collision, and the dispatcher’s
“stacking” of train routes played no role in the accident.
Perceptions of Signal Aspects
Four witnesses at the Chatsworth station stated that they had seen the westbound CP
Topanga signal as train 111 left the station and that the signal was displaying a green aspect. But,
NTSB Railroad Accident Report
National Transportation Safety Board 52
as previously noted, all the physical and documentary evidence shows conclusively that the
signal aspect was red.
The results of postaccident sight-distance tests demonstrated the difficulty in identifying
a red signal aspect at CP Topanga when viewed from the Chatsworth station. During that testing,
test participants on the station platform were able to identify green and flashing yellow signals
but were unable to reliably identify a red signal. The engineer who participated in the sight-
distance tests and who, by his own account, “knew where to look,” had to move his locomotive
almost 1,000 feet from the station before he had what he considered to be a view of the signal
adequate to positively identify the signal aspect when it was displaying red, or stop. At this
distance, some members of the observation group reported that they were still unable to reliably
identify the red aspect. These findings were not surprising given that the signal aspect is an 8
3/8-inch-diameter lighted disk almost a mile away being viewed in daylight.
Eyewitness reports of the signal indication at the time of the accident must be evaluated
in the context of the physical relationship between the signal and the station, the environmental
conditions, and the capabilities and known limitations of the human visual system. The visual
angle of the westbound signal light at CP Topanga when viewed from Chatsworth station is
essentially equal to the aperture of a single photoreceptor, which puts it near the limit of normal
visual function,
58
making it particularly difficult to identify signal color from that distance. An
observer with excellent vision who is familiar with the signal and the surrounding environment
may be able to see, and perhaps identify the color of, the signal light, but it is more likely that an
observer either will not be able to see a signal light at this distance or will misidentify its color.
As illustrated by the sight-distance testing results in this investigation, this is particularly true of
a red signal aspect because the human visual system is less sensitive to red light than green light.
Research on railroad signal detection has reported misperceptions of signal color at long
distances under certain conditions or by certain viewers.
59
However, that research was associated
with viewing distances of about 2,950 feet, which is a little more than half the distance from
Chatsworth station to CP Topanga. At longer distances, research showed that viewers were often
unable to accurately perceive signal color.
The human visual system has been found to be more sensitive to brightness than to color
when viewing very small stimuli.
60
That is, the stimulus may be above a person’s threshold for
perception of brightness but below the threshold for the perception of color, allowing a viewer to
58
Studies of the human retina estimate that at the center of the foveal region—which corresponds roughly to
the center of a person’s field of view—a single cone photoreceptor in a typical human eye integrates light through an
aperture approximately 2.5µm in diameter, equating to a visual angle of approximately 0.5 arcminutes or .008
degrees. (An arcminute is a unit of angular measurement equal to 1/60 of 1 degree.) The common visual acuity
reference of 20/20 is the ability to resolve a high contrast spatial pattern separated by 1 arcminute. For addition
information see (a) D. R. Williams. “Topography of the Foveal Cone Mosaic in the Living Human Eye,” Vision
Research 28 (1988): 433-454. (b) C. A. Curcio, K. R. Sloan, R. E. Kalina, and A. E. Hendrickson. “Human
Photoreceptor Topography,” Journal of Comparative Neurology 292 (1990): 497-523. (c) L. N. Thibos. “Formation
and Sampling of the Retinal Image,” in K. K. De Valois (Ed.) Seeing (San Diego, CA: Academic Press, 2000) pp.1-
49.
59
J. M. Wood, D. A. Atchison, and A. Chaparro. “When Red Lights Look Yellow,” Investigative
Ophthalmology and Visual Science. 46(11) (2005): 4348-4352.
60
P. E. King-Smith and D. Carden. “Luminance and Opponent-Color Contributions to Visual Detection and
Adaptation and to Temporal and Spatial Integration.” Journal of the Optical Society of America. 1976;66:709–717.

NTSB Railroad Accident Report
National Transportation Safety Board 53
perceive a lighted object without being able to identify its color. Consistent with this
phenomenon, Wood et al. found that observers could report red railroad signals as still appearing
bright at distances from which they could not perceive them as red.
61
In this accident, witnesses
viewing the signal from the station under the lighting conditions at the time may have seen the
signal, if they saw it at all, as “not red” rather than positively green and may simply have
perceived the color they expected. One of the rail fan witnesses who had reported seeing the
green signal at CP Topanga acknowledged in his interview that red signals at CP Topanga were
not visible during the day, they were visible only at night. Therefore, the NTSB concludes that
eyewitness reports of seeing a green aspect from the Chatsworth station are contrary to the other
evidence; postaccident testing and research show that witnesses could not have reliably seen the
red aspect that the CP Topanga signal was displaying as train 111 departed the station because of
a combination of extreme distance to the signal (more than 1 mile), lighting conditions at the
time, and limitations of the human visual system.
Performance of Train 111 Engineer
While at the Chatsworth station, the train 111 engineer had a view of the CP Topanga
signal that was subject to the same limitations as that of the witnesses on the platform. But unlike
the witnesses, this was not the engineer’s first clue that the signal might be red, nor was it his last
opportunity to observe, identify, and respond to it.
Both the flashing yellow aspect at CP Bernson and the solid yellow aspect at signal 4451
would have indicated to the engineer that the CP Topanga signal was red and that he would have
to stop there if the signal did not clear before he reached it. The engineer saw the flashing yellow
signal and was recorded calling it out over the radio. He was not recorded calling out the solid
yellow signal, so it cannot be confirmed whether he observed it, although he clearly had the
opportunity to do so.
Similarly, when train 111 departed Chatsworth station, the engineer had additional
opportunities to observe and respond to the signal at CP Topanga. His train was moving during
this time, so the signal would have been coming more clearly into his view as he approached it.
But he was not recorded calling out this signal over the radio, and he clearly did not respond
appropriately to the stop indication it was displaying. The engineer’s action, or lack of action,
with regard to the red stop signal at CP Topanga suggests that he was not fully attentive to his
primary task of operating his train safely. He did manipulate the train controls during this time,
but these manipulations involved long-practiced and ingrained tasks that he could carry out with
little conscious effort and without being particularly focused on his work.
Records from the engineer’s cell phone provider show activity on the engineer’s wireless
device between the time the train left the station and the time of the collision, indicating that the
device was on and being used during that period. The records show that at 4:21:03 p.m., or 47
seconds after departing the station, the engineer received a 71-character text message on his
wireless device. Sometime within the next minute he responded with a 32-character text
message. This was the last text message the engineer sent or received before the collision.
61
Wood, et. al., “When Red Lights Look Yellow,”
NTSB Railroad Accident Report
National Transportation Safety Board 54
Because wireless network records regarding “sent” times are less precise than those
regarding “received” times, it cannot be known with certainty at what time the engineer pressed
the “send” button on his wireless device to transmit his last message. But the content of the
message clearly shows that it was in response to the previous message, which he had received
just as the train was pulling out of the station. Thus, during at least part of the time that he could
have been, and should have been, observing the signal at CP Topanga, the engineer was likely
reading an incoming text message, formulating a response, and entering that response into his
wireless device.
Among highway users, text messaging has been shown to have the potential to impose
visual, manual, and cognitive demands that greatly exceed those required for voice calls.
62
Furthermore, research has demonstrated that people adjust their reading rate to accommodate the
rate at which messages scroll. As the rate of scroll increases, more time is devoted to reading and
comprehending the message, making less time available for viewing the roadway.
63
The train 111 engineer’s participation in text messaging after departing Chatsworth
station distracted him from adequately attending to a critical task—observing and properly
responding to the signal indication at Topanga. He should have known to expect a red signal
there because of the flashing yellow signal at CP Bernson that he reported and the solid yellow
signal at 4451 he had passed only moments before. He may have thought, or hoped, that the
signal would clear before his train reached it, but even this expectation would have required that
he proceed while being prepared to stop and that he continue to observe the signal until his train
reached it. He did neither. The engineer’s operation of the train throttle, bell, and horn after he
left the station, as well as his text messaging, indicated that he was alert and should have been
able to operate his train in accordance with operating rules. But evidence gathered during the
investigation suggests that, temporarily at least, the engineer was more attentive to his text
messaging and to his anticipated meeting later that evening with young rail fans than he was to
the safe operation of his train. The engineer’s deficient performance reinforces the research
findings that, in operational settings such as this, text messaging can lead to performance
decrements related to distraction and inattention.
64
The NTSB concludes that the engineer of
train 111 was actively, if intermittently, using his wireless device shortly after his train departed
Chatsworth station, and his text messaging activity during this time compromised his ability to
observe and appropriately respond to the stop signal at CP Topanga.
62
J. D. Lee. (2007). “Driver Distraction: Breakdowns of a Multi-Level Control Process,” In: I. J. Faulks, M.
Regan, M. Stevenson, J. Brown, A. Porter & J.D. Irwin (Eds.). Distracted Driving (Sydney, NSW: Australasian
College of Road Safety, 2007). Pp. 75-98.
63
J. D. Hoffman, J. D. Lee, D. V. McGehee, Department of Mechanical and Industrial Engineering, Public
Policy Center, The University of Iowa, Iowa City, IA. In: Proceedings of the Human Factors and Ergonomics
Society 50thAnnual Meeting, 2006.
64
Studies of the perceptual phenomenon known as “inattentional blindness” have demonstrated that distracted
viewers can fail to detect critical visual stimuli even when they are fixating on those stimuli. See A. Mack and I.
Rock. Inattentional Blindness (Cambridge, MA: MIT Press, 1998) for a complete discussion of the topic.

NTSB Railroad Accident Report
National Transportation Safety Board 55
Train 111 Engineer’s Use of Wireless Device
The investigation revealed that, between about 6:05 a.m. and 4:22 p.m. on the day of the
accident, the engineer sent or received a total of 95 text messages. During the time periods
(morning and evening shifts) that he was responsible for operating a train, he sent 21 text
messages, received 20 text messages, and made four outgoing telephone calls. The investigation
further revealed that this amount of activity was not unusual for this engineer. Wireless records
for the 7 days preceding the accident showed that on each workday, the engineer had sent or
received text messages or made voice calls during the time he was responsible for operating a
train. On the day with the least wireless activity, he sent or received (during his work period)
about 30 text messages. On Wednesday, 2 days before the accident, he sent or received about
125 messages during the time he was responsible for operating a train. He had also made phone
calls during these periods.
The General Code of Operating Rules and Connex operating rules forbid non-work-
related and non-emergency use of personal wireless devices by operating crewmembers. In fact,
the train 111 engineer was in violation of Connex operating rules simply by having his wireless
device in the locomotive cab and turned on while he was at the controls of the locomotive or cab
control car. But the engineer went further, from simply having the device to actually using it to
read and compose messages during the time his primary task was to operate the train safely and
to be attentive and properly responsive to all signal indications.
The engineer was well aware that he was violating company rules with regard to his use
of a wireless device. In 2006, as part of an efficiency test, he was found to have his cell phone
turned on in his briefcase. He said that he had forgotten to turn it off when he went on duty, but
he was documented at that time as having failed to comply with company safety rules. Only
about a month before the accident, the conductor on the engineer’s train saw the engineer using
his cell phone, and he reminded him of the prohibition. The conductor said the engineer
acknowledged that such use was a violation of company rules. The conductor reported the
incident to a supervisor who, according to testimony during the public hearing on this accident,
once again counseled the engineer with regard to the rule regarding use of wireless devices. The
NTSB concludes that the Metrolink engineer was aware that he was violating company safety
rules when he used his cell phone to make calls or to send and receive text messages while on
duty, but he continued the practice nonetheless.
Leesdale Local Conductor’s Use of Wireless Device
The engineer of train 111 was not the only crewmember involved in this accident to have
made prohibited use of a wireless device. The records indicate that the conductor of the Leesdale
Local sent or received a total of 41 text messages while on duty, with 35 of these being sent or
received during the time the conductor’s report shows that the train was moving. His last
outgoing text message was received and logged by the Verizon network at 4:20 p.m., about the
time his train exited tunnel 27 and about 2 minutes before the collision.
Although the conductor was in the cab of the locomotive at the time he sent his last text
message before the accident, he was not at the controls. And although he, along with the
engineer, was responsible for observing signal indications and helping ensure compliance with

NTSB Railroad Accident Report
National Transportation Safety Board 56
those indications, no evidence was found to indicate that the train handling of the Leesdale Local
was unusual or inconsistent with the signal indications the train was operating under. The NTSB
therefore concludes that, although the conductor of the Leesdale Local violated operating rules
by sending and receiving text messages during times when he shared responsibility for the safe
operations of his train, any distraction caused by such use did not cause or contribute to this
accident.
Unauthorized Persons in Locomotive Cab
The prohibition against cell phone use was not the only company safety rule the engineer
of train 111 knowingly violated. As was clear from the content of the text messages the engineer
exchanged with the young rail fan identified in this report as “Person A,” the engineer had,
earlier in the week, allowed Person A and one or more friends to board his train and join him in
the locomotive cab. The engineer apparently had allowed at least one of these individuals to
operate the train for a portion of the trip. On the day of the accident, the engineer planned to have
Person A and one or more other individuals board the locomotive at Moorpark. He further
planned to allow Person A and perhaps one or more other individuals to actually operate the train
from Moorpark to the end of the line at Montalvo. This plan was only about 3 1/2 hours from
fruition when the accident occurred.
As with wireless devices, Connex had specific rules prohibiting unauthorized persons
from occupying the locomotive cab or operating compartment of a train while the train was in
service. The engineer was obviously aware of the rules because he conspired with the rail fans to
have them board his train surreptitiously. Many of the text messages the engineer exchanged
with Person A on the afternoon of the accident had to do with the planned boarding at Moorpark,
with several comments reflecting full awareness, by both parties, that allowing unauthorized
persons to board the train, not to mention actually operating it, constituted a violation of railroad
rules.
Efficiency Testing and Management Oversight
The engineer of train 111 had been subject to efficiency and rules testing throughout his
railroad career. Nothing exceptional was found in the records of this testing. As already noted, on
two occasions in the previous 2 years he had been counseled about his use of a cell phone while
on duty, but neither instance suggested a pattern of violations or an ongoing, willful disregard for
the rules. And yet, as shown by his wireless account records (which would not have been
available to Connex managers), the engineer habitually used his cell phone at times when he
knew that any distraction from the task at hand could have serious safety consequences. Further,
by actively encouraging and facilitating access by unauthorized persons to the locomotive cab,
he created a situation that could pose another serious safety risk.
As acknowledged during the public hearing on this accident, the nature of rail operations
makes enforcement of certain operating rules extremely difficult, if not impossible. Metrolink
trains, as is common with other passenger trains, have only the engineer in the operating
compartment. No reasonable method exists for management, by personal observation, to

NTSB Railroad Accident Report
National Transportation Safety Board 57
determine whether the engineer (or other crewmember) boards the train with a personal wireless
device in his or her possession, and once the train leaves a station, no mechanism is currently in
place to determine whether the device is in use.
The conductor on train 111, who 1 month before the accident had cautioned the engineer
about his use of his cell phone while on duty and had taken the extra step of reporting the
incident to a manager, stated that he believed this to be an isolated event and that he was not
aware of the engineer’s pattern of cell phone use while on duty. The engineer clearly took
advantage of the privacy afforded by the locked locomotive cab to freely and repeatedly use his
cell phone in violation of railroad operating rules. Even though this engineer and conductor had
worked together 5 days a week, two shifts per day, for the previous 5 months, the conductor was
not aware of the extent to which the engineer was using his wireless device while aboard the
train. It is therefore unlikely that routine efficiency testing would ever have identified the scope
of the engineer’s violations with regard to wireless devices.
Similarly, the engineer’s permitting of unauthorized persons to occupy the operating
compartment of his locomotive stood a very low likelihood of being discovered through ordinary
management supervision or efficiency testing. The engineer was familiar enough with his route
and with the scope of management’s oversight to be able to violate the rules without discovery.
He had already allowed his rail fan friends one “ride-along” earlier in the week, and he knew
where, when, and how they could again board his train undetected on the evening of the
accident.
After the accident, Metrolink stiffened the penalty for unauthorized use of wireless
devices by crewmembers on moving trains. Such violations will now result in immediate
termination of employment. Similarly, with the issuance of Emergency Order 26, the FRA has
raised violations involving the use of wireless devices to the Federal level. But making the
violation more serious or the penalty more severe does not address the difficulty in identifying
violators. With regard to both cell phone use and allowing unauthorized persons into his train’s
operating compartment, the train 111 engineer obviously had a high degree of confidence that his
actions would not be detected. He already faced the prospect of severe penalties if he was caught,
especially with regard to having unauthorized persons aboard, but that threat was not sufficient
to deter him, given the low likelihood of detection.
As shown in the case of the conductor of the Leesdale Local, who also made
inappropriate use of a wireless device to send a text message only minutes before the collision,
even having other crewmembers present is an insufficient deterrent against such use.
The NTSB therefore concludes that, because of the privacy afforded by a locomotive cab
or train operating compartment, routine efficiency testing and performance monitoring practices
are inadequate to determine whether or to what extent engineers or other crewmembers may not
be complying with safety rules such as those regarding use of wireless devices or allowing
access by unauthorized persons.

NTSB Railroad Accident Report
National Transportation Safety Board 58
In-Cab Audio and Image Recording Devices
The engineer in this accident was able to conceal his inappropriate behavior because he
was aware each time he was, or could have been, observed by management. He would likely
have been deterred in his cell phone use and in his allowing access to unauthorized persons only
if he had known that his performance at the train controls was subject to review at any time, not
just when a manager was in the operating compartment or nearby. The NTSB believes that the
only reasonable and reliable mechanism for making such observations is an in-cab audio and
image recorder that will capture a crewmember’s activities while in the train operating
compartment.
The NTSB has long supported the installation of audio recording devices in locomotive
cabs or train operating compartments. In all too many accidents, the individuals directly involved
are either limited in their recollection of events or, as in the case of the Chatsworth accident, are
not available to be interviewed because of fatal injuries. In a number of accidents the NTSB has
investigated, a better knowledge of crewmembers’ actions before an accident would have helped
reveal the key causal factors and would perhaps have facilitated the development of more
effective safety recommendations.
As a result of its investigation of the collision between a Maryland Rail Commuter train
and an Amtrak train near Silver Spring, Maryland, on February 16, 1996,
65
in which no
operating crewmembers survived, the NTSB was unable to determine whether certain
crewmember activities leading up to the accident may have contributed to the accident.
Consequently, the NTSB recommended that the FRA:
R-97-9
Amend 49 Code of Federal Regulations Part 229 to require the recording of train
crewmembers’ voice communications for exclusive use in accident investigations
and with appropriate limitations on the public release of such recordings.
After its investigation of another railroad accident with no surviving crewmembers that
occurred in 1999 in Bryan, Ohio,
66
the NTSB reiterated Safety Recommendation R-97-9 to the
FRA. The FRA responded that it
has reluctantly come to the conclusion that this recommendation should not be
implemented at the present time. . . . FRA appreciates that, as time passes and other
uses are found for recording media that may create synergies with other public
and private purposes, the Board’s recommendation may warrant re-examination.
Based on this response and further meetings, the NTSB classified Safety
Recommendation R-97-9 “Closed—Unacceptable Action.”
65
Collision and Derailment of Maryland Rail Commuter MARC Train 286 and National Railroad Passenger
Corporation Amtrak Train 29 Near Silver Spring, Maryland, on February 16, 1996, Railroad Accident Report
NTSB/RAR-97/02 (Washington, DC: National Transportation Safety Board, 1997).
66
Collision Involving Three Consolidated Rail Corporation Freight Trains Operating in Fog on a Double Main
Track Near Bryan, Ohio, January 17, 1999, Railroad Accident Report NTSB/RAR-01/01 (Washington, DC:
National Transportation Safety Board, 2001).

NTSB Railroad Accident Report
National Transportation Safety Board 59
Since the refusal by the FRA to act on the recommendation regarding in-cab recorders,
the NTSB has continued to investigate accidents in which such recorders would have provided
valuable information to help determine probable cause and develop safety recommendations.
Most recently, as a result of its investigation of a July 10, 2005, collision of two CN freight trains
in Anding, Mississippi,
67
the NTSB made the following safety recommendation to the FRA:
R-07-3
Require the installation of a crash- and fire-protected locomotive cab voice
recorder, or a combined voice and video recorder, (for the exclusive use in
accident investigations and with appropriate limitations on the public release of
such recordings) in all controlling locomotive cabs and cab car operating
compartments. The recorder should have a minimum 2-hour continuous recording
capability, microphones capable of capturing crewmembers’ voices and sounds
generated within the cab, and a channel to record all radio conversations to and
from crewmembers.
Investigators in those transportation modes where such recordings are available have not
only been able to analyze voice communication between operating crewmembers in the moments
leading up to an accident, but they have also been able to review and analyze other sounds
originating from the vehicle. From such sounds, parameters such as engine rpm, system failures,
speed, and the time at which certain events occur can often be determined, leading to more
precise findings and determination of probable cause. The FRA indicated in its response to the
NTSB’s recommendation that the subject of in-cab video and audio recordings had been
discussed at a meeting of the Railroad Safety Advisory Committee Locomotive Working Group.
Pending more information about those discussions, Safety Recommendation R-07-3 was
classified “Open—Acceptable Response” on July 31, 2009.
As is clear from the wording of Safety Recommendations R-97-9 and R-07-3, the
NTSB’s emphasis up to this point has been on the use of audio and/or image recordings as a tool
of accident investigation. But this accident demonstrates that audio-only in-cab recordings that
may be reviewed only after an accident do not represent the most effective use of recorder
technology for accident prevention. Even had the Metrolink locomotive in this accident been
equipped with audio recording devices, the Metrolink engineer, with the appropriate settings on
his wireless device, would most likely have been able to continue with his text messaging
activities without the equipment having captured it.
The presence, in addition to audio recording capability, of in-cab image recording
capability would have been the only means available to have determined exactly what actions the
engineer was taking during the accident trip. These images would have revealed the engineer’s
text messaging activities even absent any sounds that could have been captured by an audio
recorder. Similarly, any entry into the locomotive or train operating compartment by
unauthorized persons would be evident on image recorders.
In accidents or incidents in which employee misbehavior is not a factor, in-cab audio and
video recordings could be used to validate train crew performance as well as identify potential
67
Collision of Two CN Freight Trains, Anding, Mississippi, July 10, 2005, Railroad Accident Report
NTSB/RAR-07/01 (Washington, DC: National Transportation Safety Board, 2007).

NTSB Railroad Accident Report
National Transportation Safety Board 60
causal or contributory system design deficiencies or equipment malfunctions that may not
evident from other available parametric data.
Some railroads have already installed one type of image recorder—a forward facing
video recorder—on their locomotives, primarily for use after grade crossing accidents. The two
locomotives of the Leesdale Local were equipped with forward-facing video recorders. The
output of those recorders was used in this accident investigation to validate the information
drawn from signal data records. Although other evidence in this accident was sufficient to show
conclusively that the engineer failed to comply with a red signal, forward-facing image and
audio recorders can often be helpful in determining not only signal aspect, but also signal
visibility, as well as identifying other external factors that may influence a train crew’s
performance in the period leading up to an accident.
But even if audio and video recording devices had been installed in the Metrolink train
111 locomotive before this accident, they would not have contributed to preventing it so long as
their output could be used only after the accident occurred. The NTSB believes that the recorded
audio and images should be easily recoverable and available for review not only after an accident
has occurred but routinely, as part of the railroad’s efficiency testing and performance
monitoring program.
68
In the same way that operating employees are continually tested on signal
compliance or speed control, audio and image recordings of engineers and other crewmembers
could be reviewed at random to verify compliance with safety rules and procedures. In particular,
this information could allow railroads to identify unsafe behaviors and pursue corrective action
before an accident occurs. Further, an employee who is aware that his or her activities in the train
control compartment are subject to review by management will be much less likely to engage in
conduct—such as using a wireless device or allowing unauthorized persons in the locomotive
cab—that could lead to an accident. Even if an employee is not discouraged from performing
these or other unsafe acts, detection of those behaviors would prompt corrective actions that
would improve safety. Additionally, not all actions or conditions that have safety implications
involve employee misconduct or rules violations. Regular review of in-cab audio and image
recordings would give managers insight into other potential safety issues or unsafe operating
practices that may not be revealed by any other means and of which the crews themselves may
be unaware. Action could then be taken to address these issues through changes in rules,
operating practices, or employee training programs.
The NTSB therefore concludes that a train crew performance monitoring program that
includes the use of in-cab audio and image recordings would serve as a significant deterrent to
the types of noncompliance practices with safety rules engaged in by the Metrolink engineer and
the UP Leesdale Local conductor in this accident and would provide railroads with a more
comprehensive means to evaluate the adequacy of their safety programs.
To be effective, any such recording devices must be capable of capturing crewmember
activities during a wide range of operating conditions and over a considerable period of time.
The image recorders should have a resolution and frame rate sufficient to capture crew
movements under typical operating conditions, which includes daylight, night, and conditions of
68
As detailed in appendix B, the NTSB has, in all transportation modes, long advocated the use of recorded
data not only for accident investigation, but also for safety management and employee oversight.

NTSB Railroad Accident Report
National Transportation Safety Board 61
varying sun angles.
69
The duration of the recording should be at least 12 hours. Railroad
crewmembers may be on duty for up to 12 hours, and their actions or inactions at any time
during that period could set the stage for an accident. Also, from the standpoint of efficiency
testing or performance monitoring, the more information that is available to management, the
more likely it is that the company can assess the performance of its people or the effectiveness of
its training.
The NTSB therefore recommends that the FRA require the installation, in all controlling
locomotive cabs and cab car operating compartments, of crash- and fire-protected inward- and
outward-facing audio and image recorders capable of providing recordings to verify that train
crew actions are in accordance with rules and procedures that are essential to safety as well as
train operating conditions. The devices should have a minimum 12-hour continuous recording
capability with recordings that are easily accessible for review, with appropriate limitations on
public release, for the investigation of accidents or for use by management in carrying out
efficiency testing and systemwide performance monitoring programs. Because this
recommendation expands upon and reinforces the intent of Safety Recommendation R-07-3, that
recommendation is reclassified “Closed—Unacceptable Action/Superseded.”
If image and audio recordings are to be used to prevent, and not simply to reconstruct,
accidents, railroad managers must be authorized to review the recordings regularly as part of
their programs of efficiency testing and performance monitoring of train crews. The NTSB
therefore recommends that the FRA require that railroads regularly review and use in-cab audio
and image recordings (with appropriate limitations on public release), in conjunction with other
performance data, to verify that train crew actions are in accordance with rules and procedures
that are essential to safety.
Concerns about individual privacy have typically influenced decisions about the
installation and use of audio or image recorders to record crewmembers at work. However, the
NTSB does not believe that employee privacy should take precedence over public safety given
the many accidents and incidents, in all transportation modes, that the NTSB has investigated
that involved vehicle operator distraction. Workers in safety-critical positions in all industries
should expect to be observed in the workplace, just as most employees should expect their
employers to be able to monitor such activities as e-mail and Web browsing during work hours.
The argument for complete privacy in settings such as a locomotive cab, where lives of many are
entrusted to the care of one, is not persuasive.
The NTSB notes that, since the accident, SCRRA has installed inward- and forward-
facing cameras in its Metrolink locomotives to monitor engineer compliance with rules regarding
electronic devices, unauthorized personnel, and sleeping on duty.
69
International specifications for aircraft accident investigation recorders state a minimum frame rate of 4
images per second and overall resolution sufficient to distinguish between parallel 5mm resolution bars on a
standard image resolution chart. Source: Minimum Operational Performance Specification for Crash Protected
Airborne Recorder Systems, ED-112 (Paris: The European Organisation for Civil Aviation Equipment, 2003).

NTSB Railroad Accident Report
National Transportation Safety Board 62
Metrolink Passenger Survivability
For those passengers in the first coach who were in the section of the railcar that was
subject to the telescoping action, the accident was generally not survivable. For those passengers
who were occupying the area just behind the telescoped section but in front of the rear
vestibule/stairwell area, the accident was borderline survivable, although most of those
individuals who survived sustained injuries either because of the deceleration forces or from
interaction with elements of the car that were crushed. For those passengers occupying the
section of the first railcar that was not subject to the telescoping action (that is, the part aft of the
rear vestibule/stairwell), the risk of injury came from the substantial deceleration forces that their
bodies absorbed.
The occupants of the second and third passenger coaches experienced essentially no loss
of occupant survival space, but they, too, were at risk of injury from deceleration forces. The
magnitude of these forces decreased with distance from the point of impact. The NTSB
concludes that passenger survivability in this accident was determined almost exclusively by
where an individual was located, and the extremely high collision forces resulted in a loss of
occupant survival space in the forward two-thirds of the first passenger coach.
For the type of passenger coach involved in this accident, the FRA has issued minimum
static end-loading strength and crashworthiness requirements. Based on documentation reviewed
as part of this accident investigation, the design of the BiLevel railcars involved in this accident
was in compliance with FRA regulatory requirements. Also, during the physical inspection of the
damaged equipment and subsequent review of FRA compliance certification documentation,
nothing was found to suggest that the coaches were not built to FRA standards.
The NTSB does have a concern, however, about the workstation tables that are situated
throughout the BiLevel coaches. These tables (four tables on the upper level and two at each
intermediate level) are fitted between paired sets of passenger seats. As configured, these one-
piece tabletops are at abdomen height for a passenger seated at the table, thus placing that person
at risk of sustaining serious abdominal injury in the event of a high-g deceleration (such as a
collision impact).
As a result of its investigation of the 2002 collision of a Metrolink commuter train with a
Burlington Northern Santa Fe freight train in Placentia, California,
70
the NTSB determined that
two Metrolink passengers had been fatally injured as a result of abdominal injuries resulting
from impact with a workstation table. The investigation also identified research undertaken by
the FRA, using resources of the Volpe National Transportation Systems Center and other
organizations, to address collision-induced injury resulting from these workstation tables. This
research has resulted in some prototype designs for further evaluation. In the meantime, SCRRA
has indicated to the NTSB that it is purchasing Crash Energy Management cab control cars and
trailer cars that will be placed in operation starting in 2010. These cars will have crash-energy
seats, frangible tables, and push-back couplers. Existing Metrolink coaches will also be
retrofitted with these same features. The NTSB is encouraged by the progress being made in this
70
Collision of Burlington Northern Santa Fe Freight Train With Metrolink Passenger Train, Placentia,
California, April 23, 2002, Railroad Accident Report NTSB/RAR-03/04 (Washington, DC: National Transportation
Safety Board, 2003).

NTSB Railroad Accident Report
National Transportation Safety Board 63
area by the FRA, SCRAA, and others and will continue to monitor developments that reduce the
risk of injury and death to rail passengers during an accident.
Positive Train Control
The accident at Chatsworth was the second accident involving a collision between a
freight train and a Metrolink passenger train that the NTSB has investigated. In the previously
referenced investigation into the 2002 collision in Placentia, California, the NTSB determined
that the eastbound Burlington Northern Santa Fe freight train failed to comply with an approach
signal indication and was therefore unable to stop short of the next signal, which was displaying
a stop indication. The train continued past the stop signal and collided head-on with a Metrolink
passenger train. The accident resulted in 2 fatalities and more than 100 injuries.
The NTSB has long advocated the implementation of positive train control systems that
would prevent train-to-train collisions such as those that occurred at Placentia and Chatsworth.
Over the past 4 decades, the NTSB has investigated a multitude of railroad accidents that could
have been avoided through use of a positive train control system that will automatically assume
some control of a train if the crew does not comply with a signal indication. The NTSB
concludes that had a fully implemented positive train control system been in place on the
Ventura Subdivision at the time of this accident, it would have intervened to stop Metrolink train
111 before the engineer could pass the red signal at CP Topanga, and the collision would not
have occurred.
Positive train control was on the NTSB’s Most Wanted List of Transportation Safety
Improvements since the list’s inception in 1990. The NTSB’s many investigations of train
collisions have resulted in the issuance of a number of safety recommendations, the most recent
of which was issued as a result of the investigation of a collision involving three freight trains in
Bryan, Ohio.
71
That recommendation, issued to the FRA, was as follows:
R-01-6
Facilitate actions necessary for development and implementation of positive train
control systems that include collision avoidance, and require implementation of
positive train control systems on main line tracks, establishing priority
requirements for high-risk corridors such as those where commuter and intercity
passenger railroads operate.
In its report on the 2002 accident in Placentia, California, the NTSB reiterated Safety
Recommendation R-01-6 to the FRA. While disappointed in the time that has elapsed since the
issuance of the recommendation, with little effective action by the FRA, the NTSB notes that the
Rail Safety Improvement Act of 2008 mandates that not later than 18 months from the date of
enactment, Class I railroads shall develop and submit to the Secretary of Transportation a plan
for implementing a positive train control system by December 31, 2015. The date of enactment
71
Collision Involving Three Consolidated Rail Corporation Freight Trains Operating in Fog at Bryan, Ohio,
January 17, 1999, Railroad Accident Report NTSB/RAR-01/01 (Washington, D.C.: National Transportation Safety
Board, 2001).

NTSB Railroad Accident Report
National Transportation Safety Board 64
was October 16, 2008, making the required date for submission of plans April 16, 2010. This
mandate will apply to Metrolink trackage in the accident area.
The NTSB is further encouraged that SCRRA is already engaged in the development and
deployment of positive train control on the Metrolink locomotive fleet by December 2012, with
the installation of positive train control on the entire SCRRA territory projected for completion
by 2015.
NTSB Railroad Accident Report
National Transportation Safety Board 65
Conclusions
Findings
1. The following were neither causal nor contributory to this accident: weather, fatigue, the
engineer’s medical conditions or treatments, training and experience of crewmembers,
operation of Union Pacific Leesdale Local, alcohol or illegal drug use by operating
crewmembers, and condition of the track or rolling stock.
2. Although the conductor of the Union Pacific Leesdale Local had likely used marijuana
within 3 to 11 hours of the accident, this was neither causal nor contributory to the accident.
3. Considering the challenges of the recovery operations, the emergency response to the
accident was timely, well coordinated, and effectively managed.
4. Because locomotive cab exits are not designed to be quickly opened in an emergency,
firefighters could not rapidly enter the cab of the Union Pacific Leesdale Local to rescue the
injured crew.
5. Physical evidence, documentary and recorded data, and postaccident signal examination and
testing confirm that the westbound signal at Control Point Topanga was displaying a red
aspect at the time Metrolink train 111 departed Chatsworth station and as it approached and
passed Control Point Topanga, and had the engineer complied with this signal indication, the
accident would not have occurred.
6. Eyewitness reports of seeing a green aspect from the Chatsworth station are contrary to the
other evidence; postaccident testing and research show that witnesses could not have reliably
seen the red aspect that the Control Point Topanga signal was displaying as train 111
departed the station because of a combination of extreme distance to the signal (more than 1
mile), lighting conditions at the time, and limitations of the human visual system.
7. The signal and traffic control systems worked as designed on the day of the collision, and the
dispatcher’s “stacking” of train routes played no role in the accident.
8. The engineer of train 111 was actively, if intermittently, using his wireless device shortly
after his train departed Chatsworth station, and his text messaging activity during this time
compromised his ability to observe and appropriately respond to the stop signal at Control
Point Topanga.
9. The Metrolink engineer was aware that he was violating company safety rules when he used
his cell phone to make calls or to send and receive text messages while on duty, but he
continued the practice nonetheless.

NTSB Railroad Accident Report
National Transportation Safety Board 66
10. Although the conductor of the Union Pacific Leesdale Local violated operating rules by
sending and receiving text messages during times when he shared responsibility for the safe
operations of his train, any distraction caused by such use did not cause or contribute to this
accident.
11. Because of the privacy afforded by a locomotive cab or train operating compartment, routine
efficiency testing and performance monitoring practices are inadequate to determine whether
or to what extent engineers or other crewmembers may not be complying with safety rules
such as those regarding use of wireless devices or allowing access by unauthorized persons.
12. A train crew performance monitoring program that includes the use of in-cab audio and
image recordings would serve as a significant deterrent to the types of noncompliance
practices with safety rules engaged in by the Metrolink engineer and the Union Pacific
Leesdale Local conductor in this accident and would provide railroads with a more
comprehensive means to evaluate the adequacy of their safety programs.
13. Passenger survivability in this accident was determined almost exclusively by where an
individual was located, and the extremely high collision forces resulted in a loss of occupant
survival space in the forward two-thirds of the first passenger coach.
14. Had a fully implemented positive train control system been in place on the Ventura
Subdivision at the time of this accident, it would have intervened to stop Metrolink train 111
before the engineer could pass the red signal at Control Point Topanga, and the collision
would not have occurred.
Probable Cause
The National Transportation Safety Board determines that the probable cause of the
September 12, 2008, collision of a Metrolink commuter train and a Union Pacific freight train
was the failure of the Metrolink engineer to observe and appropriately respond to the red signal
aspect at Control Point Topanga because he was engaged in prohibited use of a wireless device,
specifically text messaging, that distracted him from his duties. Contributing to the accident was
the lack of a positive train control system that would have stopped the Metrolink train short of
the red signal and thus prevented the collision.

NTSB Railroad Accident Report
National Transportation Safety Board 67
Recommendations
As a result of its investigation of the September 12, 2008, collision of Metrolink train 111
with Union Pacific LOF65–12 at Chatsworth, California, the National Transportation Safety
Board makes the following safety recommendations:
New Recommendations
To the Federal Railroad Administration:
Require the installation, in all controlling locomotive cabs and cab car operating
compartments, of crash- and fire-protected inward- and outward-facing audio and
image recorders capable of providing recordings to verify that train crew actions
are in accordance with rules and procedures that are essential to safety as well as
train operating conditions. The devices should have a minimum 12-hour
continuous recording capability with recordings that are easily accessible for
review, with appropriate limitations on public release, for the investigation of
accidents or for use by management in carrying out efficiency testing and
systemwide performance monitoring programs. (R-10-1)
Require that railroads regularly review and use in-cab audio and image recordings
(with appropriate limitations on public release), in conjunction with other
performance data, to verify that train crew actions are in accordance with rules
and procedures that are essential to safety. (R-10-2)
Previously Issued Recommendation Reclassified in This Report
To the Federal Railroad Administration:
R-07-3
Require the installation of a crash- and fire-protected locomotive cab voice
recorder, or a combined voice and video recorder, (for the exclusive use in
accident investigations and with appropriate limitations on the public release of
such recordings) in all controlling locomotive cabs and cab car operating
compartments. The recorder should have a minimum 2-hour continuous recording
capability, microphones capable of capturing crewmembers’ voices and sounds
generated within the cab, and a channel to record all radio conversations to and
from crewmembers.
Safety Recommendation R-07-3, previously classified “Open—Acceptable Response,” is
reclassified “Closed—Unacceptable Action/Superseded.” Safety Recommendation R-07-3 is
superseded by Safety Recommendation R-10-1.

NTSB Railroad Accident Report
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
DEBORAH A.P. HERSMAN CHRISTOPHER A. HART
Chairman Vice Chairman
ROBERT L. SUMWALT
Member
Adopted: January 21, 2010
Chairman Hersman filed the following concurring statement and was joined by Vice
Chairman Hart and Member Sumwalt.
National Transportation Safety Board 68

NTSB Railroad Accident Report
National Transportation Safety Board 69
Chairman Deborah A.P. Hersman, Concurring Statement,
Vice Chairman Christopher A. Hart and Board Member Robert L. Sumwalt,
joining in:
On January 21, 2010, by a 3-0 vote, we adopted the report on the collision of a Metrolink
passenger train with a Union Pacific freight train in Chatsworth, CA. This action concluded our
sixteen-month investigation into the September 12, 2008, collision that took 25 lives and injured
135.
As our report concludes, the probable cause of the collision was the failure of the
Metrolink engineer to comply with the red signal at Control Point Topanga because he was
texting on his personal wireless device, in violation of company policy. Distracted from his
duties, he did not stop the train and collided head-on with the approaching freight train. He did
so, despite earlier track signals and radio calls indicating he would need to stop. Contributing to
the accident was the lack of a positive train control (PTC) system that would have stopped the
train short of the red signal and thus prevented the collision.
In order to protect the safety of the traveling public, we reluctantly move further in this
report, in terms of reducing privacy in the train cab, than we ever have before. We recommend
that the Federal Railroad Administration (FRA) require the installation of audio and video
recorders in train cabs for use in accident investigations and by management in carrying out
efficiency testing and performance monitoring programs, and require railroads to regularly
monitor these recorders to ensure employees are following the safety rules.
Sensitive to privacy concerns, we have endeavored to respond to the inappropriate use of
cell phones and other wireless devices in ways that minimize intrusions of privacy. The Safety
Board's efforts in this area date back to May 2002, with an accident in Clarendon, TX, in which
an engineer was using his cell phone during the time he should have been reading a track warrant
notifying him to stop the train. This led to a head-on collision with an oncoming train. As a
result, the Safety Board recommended that the Federal Railroad Administration (FRA) issue
regulations to control the use of cell phones and similar wireless communication devices by
railroad operating employees while on duty. For more than 5 years, the FRA failed to address
this issue -- until one month after the Chatsworth accident when it issued an emergency order
restricting the use of cell phones and other distracting electronic devices by on-duty railroad
operating employees. More recently, in May of 2009, the Safety Board investigated a collision
involving two trolleys in Boston, MA. The operator of the striking train admitted to local
authorities that he was texting his girlfriend in the moments immediately prior to the collision. In
our Chatsworth investigation, records showed that the Metrolink engineer habitually violated
company policy, such as the ban on the use of cell phones while on duty. On the day of this
accident, he made four outgoing phone calls while he was on duty, and he sent or received 95
text messages, 41 of which were while he was on duty, including one 22 seconds before the
collision. Also contrary to company policy, the engineer actively facilitated unauthorized persons
to access the locomotive cab, and on at least one occasion, even allowed a minor to take the
controls. Although he had been subject to efficiency and rules testing throughout his career and
been counseled by management twice on his improper cell phone use, this inappropriate behavior
continued.

NTSB Railroad Accident Report
National Transportation Safety Board 70
Meanwhile, although not contributing to the accident, the conductor of the UP train was
also texting moments before the collision. These were two different employees, working for two
different companies, on two different trains. Our report concluded that, among other things,
because of the privacy afford by a locomotive cab, Metrolink's routine efficiency testing and
performance monitoring practices were inadequate to prevent the accident engineer from
engaging in inappropriate behaviors.
This is a watershed investigation for the Safety Board. Some may have concerns that the
recommendations in this report are over-reaching, that they impinge upon individual privacy, and
that the oversight footprint is too broad. We uniformly disagree. The Safety Board has long
supported the installation of audio recording devices in locomotive cabs for investigative
purposes. Recommendations regarding audio recorders in locomotive cabs have been on our
Most Wanted Listed and have been closed and reissued over the years, but the FRA has not acted
on these recommendations. Furthermore, what this and other accidents have shown is that
traditional forms of oversight are not working.
The Safety Board's history is filled with examples where significant accidents have
resulted in significant change. In the early 1980's, the Safety Board began recommending the use
of drug and alcohol testing for rail personnel. However, it wasn't until two major rail accidents in
the late 1980's that Congress stepped in and decided that the societal benefits of mandatory
testing outweighed any privacy concerns. Similarly, the Board has been pushing for PTC, or
some version of it, for over 30 years. Finally, after this accident, Congress again stepped it to
pass a bill requiring railroads to install PTC systems on passenger and certain hazmat routes by
the end of 2015. Sadly, it took 25 more lives and an act of Congress to finally move PTC, on
passenger rail lines, from testing to reality.
Technology is a game changer - and our Chatsworth recommendations recognize this.
Today, video recorders are everywhere, and we accept them. Video cameras record us at the
ATM and record bank tellers at work. Whether we are in a casino in Las Vegas or at Walmart,
there are cameras recording our every move. Even our Board meetings are webcast so that others
may observe our work and monitor how well we are doing our job.
In transportation, we have long accepted cameras for safety, surveillance and security. In
many cities, our children and their bus drivers are recorded on school buses for behavioral
reasons. Airports have cameras recording activities inside and outside of the terminals. At the
Safety Board, we often use video provided by airports to identify crash sequences. Trains such as
the freight train involved in this accident have been equipped with outward facing cameras
mounted on the locomotives to record, among other things, grade crossing accidents. Motor
coaches have inward facing cameras, which we have used in our investigations to correlate
driver actions, vehicle performance and evidence from the roadway. There are even cameras
photographing traffic light violators.
On a daily basis, we use technology to monitor the machines - the health of the
equipment, any needed maintenance, time between overhauls, and total cycles. We now have a
corresponding obligation to use that technology to monitor the people operating the machines.
The rail industry still relies on an extra person in the cab to monitor whether engineers are
following safety rules. Because accidents such as Chatsworth are demonstrating not only that
prohibitions have not been effective, but that monitoring the prohibitions has also not been

NTSB Railroad Accident Report
National Transportation Safety Board 71
effective, we can, and must, exploit technological advances in equipment and communications to
remedy this.
The Safety Board is an independent agency. Our mandate is to investigate accidents,
determine their probable causes, and issue recommendations to prevent them from happening in
the future. We are a safety organization, and our mission is to make transportation safer for the
travelling public. We cannot, however, do this work alone. While the Safety Board can
constantly raise the bar, it is incumbent upon our partners, -- industry, labor and the regulators -
to take the next step and implement our recommendations.
The Safety Board's work on this accident investigation has opened a lot of eyes. What we
are recommending recognizes that technology brings problems but technology also provides
solutions. We did not make these recommendations lightly. In reconciling our concerns
regarding privacy, we note that Congress has charged the Safety Board to identify safety
deficiencies and make recommendations to improve safety. It is a responsibility that we take
seriously.
Yes, it's an intrusion. Yes, it affects privacy. But when individual behaviors endanger the
lives of the travelling public, we are obligated to do everything possible to ensure their safety.
Just as we cannot turn a blind eye to that responsibility, however, neither can management turn a
blind eye to the behavior of bad actors who are not doing their job. Management is, and must be
held, accountable for the performance of their employees.
Professionalism is doing the right thing when nobody is watching. But as the Chatsworth
investigation uncovered, this particular engineer was not likely to do the right thing unless he
thought somebody was watching. This is a new paradigm, this area of distractions. It is changing
how humans behave, how they interact with one another, and how they react in normal and
emergency situations.
Our recommendations from this accident will make some people uncomfortable. They
may even make some people angry. But it is not the Safety Board's job to recommend the easy
things. It is the Safety Board's job to be a catalyst for change and to raise the bar. If we are
serious about addressing distractions in the operating environment and serious about putting
safety first, then we must put the collective ahead of the individual. We believe our
recommendations are a step in that direction.

NTSB Railroad Accident Report
National Transportation Safety Board 72
Appendix A: Investigation
Notification
The National Response Center notified the NTSB of the accident about 7:45 p.m. on
September 12, 2008. The investigator-in-charge and other members of the NTSB investigative
team were launched from the Washington, D.C., headquarters office and from the Chicago,
Illinois; Gardena, California; and Jacksonville, Florida; field offices. The NTSB’s investigation
focused on all aspects of the accident, including operations, track, signals, mechanical, human
performance, survival factors, crashworthiness, event recorder, and cellular telephone issues. The
on-scene investigation was completed on September 20, 2008.
Member Kathryn O’Leary Higgins was the Board Member on scene. Safety Board
investigators returned to the Chatsworth, California, area for follow-on investigative activities
during October and November 2008 and January 2009.
Parties to the Investigation
Participating in the investigation were the FRA, Metrolink, Connex Railroad, LLC,
Union Pacific Railroad, California Public Utilities Commission, Brotherhood of Locomotive
Engineers and Trainmen, United Transportation Union, Los Angeles Police Department, Los
Angeles Fire and Rescue, Bombardier Transportation Corporation, and Mass Electric
Construction Company.
Public hearing
A public hearing on this accident was held at the NTSB Conference Center on March 3–
4, 2009. Representatives of all parties to the investigation participated in the hearing.

NTSB Railroad Accident Report
National Transportation Safety Board 73
Appendix B: Recommendation History on
Employee Performance Monitoring
The NTSB has, in rail
72
as well as in other modes of transportation, long advocated the
use of recorded data not only for accident investigation, but also for safety management and
employee oversight. For example, in its investigation of the November 6, 1993, collision of the
passenger ship Noordam with the Maltese bulk carrier Mount Ymitos near the entrance to the
Mississippi River,
73
the NTSB found deficiencies in bridge watchstanding. As a result, the
NTSB recommended that the U.S. Coast Guard require the installation of voyage event recorders
(VERs) on all vessels over 1,600 gross tons operating in U.S. waters (Safety Recommendations
M-95-5 and -6). The NTSB noted that, when used for management oversight, VERs (also known
as voyage data recorders, or VDRs) would help prevent accidents, and that when used for
accident reconstruction, VERs would help investigators determine what measures will promote
greater safety in the future.
In its investigation of the July 16, 2004, multi-vehicle accident near Chelsea, Michigan,
74
the NTSB found that the accident was initiated when the driver of a tractor-semitrailer
combination failed to stop upon encountering traffic congestion in a temporary traffic control
zone, likely due to reduced alertness because of a failure to obtain adequate rest. The driver’s
hours of service at the time of the accident exceeded Federal limits by 5.75 hours. Contributing
to the accident were motor carrier’s insufficient regard for, and oversight of, driver compliance
with Federal hours-of-service regulations, and the failure of the Federal Motor Carrier Safety
Administration’s (FMCSA) to require motor carriers to use tamperproof driver’s logs. In its
investigation of the accident, the Safety Board determined that data from the electronic on-board
recorder (EOBR) in the accident tractor were instrumental in the reconstruction of events leading
to the accident and in the assessment of the accident driver’s hours-of-service status. Because of
the value of these data and the deficiencies identified in the FMCSA’s hours-of-service
compliance review program, the NTSB concluded that carriers should use EOBRs to verify
compliance for all operators subject to hours-of-service regulations. Therefore, in 2007, the
NTSB recommended that the FMCSA require all interstate commercial vehicle carriers to use
EOBRs so that the carriers and their regulators could monitor and assess hours-of-service
compliance (Safety Recommendation H-07-41).
The NTSB’s investigation into a number of aviation accidents also prompted
recommendations related to the use of accident recorders for operational oversight by safety
managers. For example, in its investigation of the October 14, 2004, crash of Pinnacle Airlines
72
For example, see NTSB Safety Recommendations R-81-65, R-81-67, R-84-38, R-87-21, and R-90-17.
73
Collision of the Netherlands Antilles Passenger Ship Noordam and the Maltese Bulk Carrier Mount Ymitos
in the Gulf of Mexico November 6, 1993, Marine Accident Report NTSB/Mar-95/01 (Washington, DC: National
Transportation Safety Board, 1995).
74
Rear-End Chain Reaction Collision, Interstate 94 East, Near Chelsea, Michigan, July 16, 2004, Highway
Accident Brief NTSB/HAB-07/01 (Washington, DC: National Transportation Safety Board, 2007).

NTSB Railroad Accident Report
National Transportation Safety Board 74
flight 3407 near Jefferson City, Missouri,
75
the NTSB found repeated instances of unprofessional
conduct by flight crews during repositioning flights when no passengers or cabin attendants were
on board. This behavior occurred for a number of reasons, including the crews’ perception of a
low risk of detection. As a result, the NTSB recommended that the Federal Aviation
Administration require those regional air carriers having the capability to review flight data
recorder data from nonrevenue flights to use that data to verify that flights are being conducted in
accordance with standard operating procedures (Safety Recommendation A-07-7).
Most recently, the NTSB noted that a flight operations monitoring program, had it been
in place, may have helped prevent the collision of two helicopters carrying out helicopter
emergency medical services flights in Flagstaff, Arizona, on June 29, 2008. The two Bell 407
helicopters collided in midair while approaching the Flagstaff Medical Center helipad. The
NTSB determined that the probable cause of this accident was that the two pilots failed to see
and avoid each other as their aircraft approached the helipad. Contributing to the accident were
the failure of one of the pilots to follow arrival and noise abatement guidelines and the failure of
the other pilot to follow communication guidelines. The NTSB concluded that the systematic
monitoring of data from helicopter emergency medical services flights could provide operators
with objective information regarding the manner in which their pilots are conducting these
flights. The NTSB further concluded that a periodic review of such information, along with other
available information such as pilot reports and medical crew feedback, could assist operators in
detecting and correcting unsafe deviations from company operating procedures. As a result, the
NTSB recommended that the FAA require helicopter emergency medical services flight
operators to install flight data recording devices and establish a structured flight data
management program that reviews all available data sources to identify deviations from
established norms and procedures and other potential safety issues (Safety Recommendation A-
09-90).
75
Crash of Pinnacle Airlines Flight 3701, Bombardier CL-600-2B19, N8396A, Jefferson City, Missouri,
October 14, 2004, Aircraft Accident Report NTSB/AAR-07/01 (Washington, DC: National Transportation Safety
Board, 1995).
